
Acromioclavicular ‘Pseudo-dislocation’ with Concomitant Coracoid Process Fracture and Coracoclavicular Ligament Rupture in a 12-year-old Male
Robert A. Duerr, MD, Patricia R. Melvin, MD, MBS, Dennis J. Phillips, MD
The authors report no conflict of interest related to this work.
©2018 by The Orthopaedic Journal at Harvard Medical School
 PDF
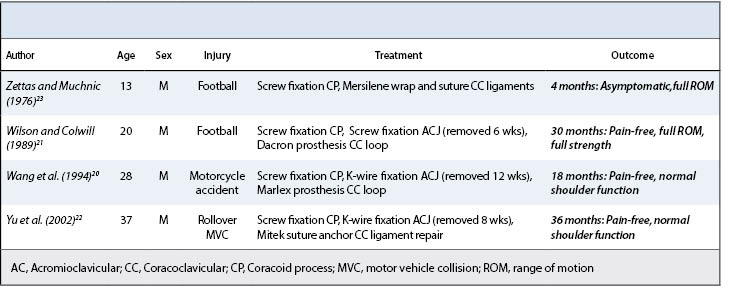
PDFINTRODUCTION The combination of lateral clavicle physeal separation (or Acromioclavicular joint dislocation), base of the coroacoid fracture, and rupture of the coracoclavicular ligaments is exceedingly rare. There is one previous case reported in a child and three similar cases reported in adults in the English-language literature.
CASE PRESENTATION A 12-year-old caucasian male presented with an acute injury to his right shoulder from a direct blow to the superolateral shoulder. Radiographs demonstrated >200% complete separation of the distal clavicle physis, and a fracture through the base of the coracoid process. Intra-operatively, the coracoclavicular ligament was found to be avulsed from the coracoid process as well. After surgical fixation of the injuries, the patient made a full recovery and at 6 months post-operatively was released to full sporting activities. At 12 months post-operatively the patient had returned to baseball as a pitcher.
CONCLUSION The shoulder suspensory complex is an important anatomic structure that enables a wide range of functional motion while maintaining connection of the upper extremity to the axial skeleton. Injury to this area is common, though often one or two areas of the complex are disrupted. As in this case, it is rare that three areas of the complex are injured in such a pattern.
LEVEL OF EVIDENCE Case Report Level V
KEYWORDS Pediatrics, trauma, AC joint
Acromioclavicular joint (AC) separations represent 10% of all shoulder injuries and 41% of sports-related shoulder injuries in adults.1,2 In children, aged 16 and below, these injuries occur less frequently and complete dislocation of the AC joint is very rare.3 In the skeletally immature, these injuries are more likely to be physeal fractures with separation of the lateral clavicular metaphysis from the epiphysis and periosteal sleeve while the stronger AC ligaments remain attached to the perichondrium of the epiphysis, termed a ‘pseudo-dislocation’.4 Dameron and Rockwood5 classified these injuries in a similar manner to AC dislocations, based on displacement of the lateral clavicular metaphysis and disruption of the periosteal sleeve.5 While this classification system is comprehensive, variations to these injury patterns have been reported.6-12 The combination of lateral clavicular physeal separation (or AC joint dislocation), base of the coracoid fracture, and rupture of the coracoclavicular (CC) ligaments, a so-called ‘triple injury’, is exceedingly rare.6 There is one previous case reported in a child and three similar cases reported in adults in the English-language literature (Table 1).6-9 The purpose of this article is to present a case report of this ‘triple injury’ and a review of the literature, mechanism of injury, and treatment.
Informed consent was obtained from this patient’s legal guardian for publication. A 12-year-old right-hand dominant male presented with pain and functional impairment of his right shoulder. Four days prior he was riding a scooter and struck a curb, causing him to flip over the handle bars at a high rate of speed, landing directly on the right shoulder and side of his head. He was initially seen in the emergency department, required several staples for a scalp laceration, and was referred for out-patient orthopedic evaluation. Physical examination demonstrated a prominent distal clavicle with swelling and tenderness to palpation around the AC joint and at the coracoid process. Both active and passive shoulder range of motion were limited due to pain. Neurovascular examination was normal. Radiographs revealed complete separation of the AC joint with >200% displacement of the distal clavicle, and a fracture through the coracoid process (Figure 1 and Figure 2).
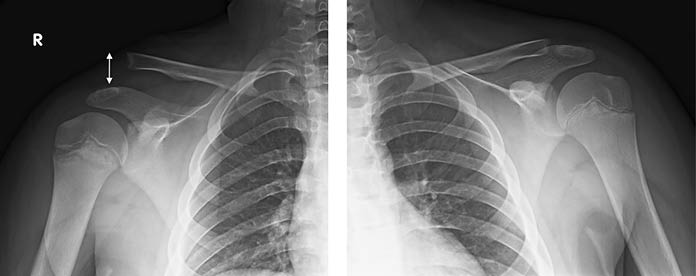
Demonstrates ≥200% displacement of the Right distal clavicle (white double arrow). The Left shoulder is shown for comparison.

Demonstrates fracture through the base of the coracoid process (white arrow)
Given the amount of displacement of the distal clavicle and fracture at the base of the coracoid, surgical treatment was recommended. At the time of surgery, the CC ligaments were found to be attached to the clavicle, although avulsed from the coracoid process. The coracoid process was fractured at the base along the physis and angulated inferiorly due to the pull of the intact conjoined tendon. The distal clavicle had separated at the physis with the epiphysis, AC ligaments, and a small sleeve of periosteum remaining attached to the acromion (Figure 3). The coracoid was reduced and a 50 mm – 4.0 cannulated partially threaded lag screw was placed. Two holes were drilled from superior to inferior in the distal clavicular metaphysis and two Fiber Wire sutures (Arthrex, Naples, FL) were passed transosseous. The distal clavicle was reduced and held in place by smooth Kirschner wires (K-wires) while the AC ligaments were repaired to the distal clavicle with the transosseous Fiber Wire sutures. Two double loaded Suture Tak anchors (Arthrex) were placed into the coracoid process at the avulsion site of the CC ligaments. The trapezoid and conoid ligaments were repaired to their respective insertion sites with the Suture Tak anchor sutures. The K-wires were removed, and the reduction remained stable (Figure 4 and Figure 5).
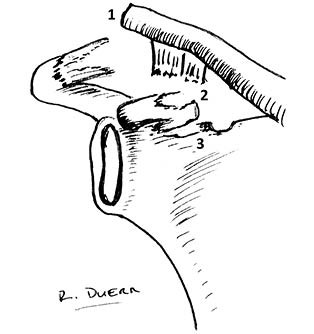
1. Distal clavicle physeal separation
2. Coracoclavicular ligament avulsed from insertion at coracoid
3. Fracture at the base of the coracoid
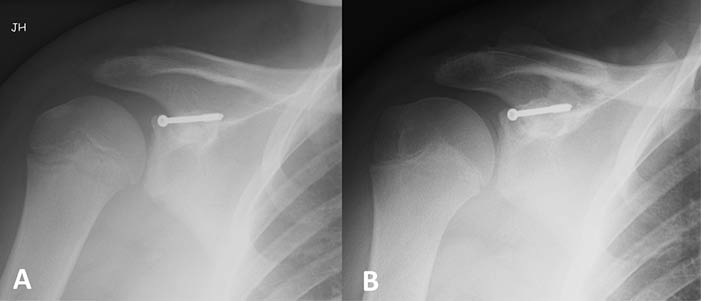
A. 2-week post-operative radiograph of the right shoulder demonstrates reduction of the AC joint. A partially threaded screw is traversing the coracoid from its tip through the fracture at the base and into the body of the scapula. B. 10-week post-operative radiograph demonstrates maintenance of the reduction and screw position.
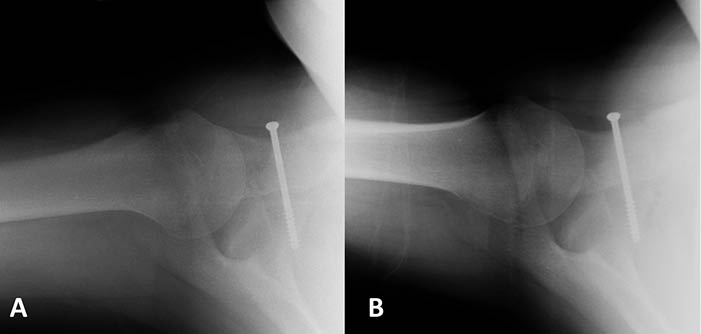
A. 2-week post-operative axillary lateral radiograph of the right shoulder demonstrates reduction of the AC joint. The partially threaded screw is traversing the coracoid process. B. 10-week post-operative radiograph demonstrates maintenance of the reduction and screw position.
Postoperatively, the patient was immobilized in a sling for six weeks with instruction to begin passive pendulum exercises at two weeks. At six weeks, the patient was pain-free and was removed from the sling to begin formal physical therapy for range of motion and strengthening. Post-operative radiographs at 10-weeks (Figure 4 and Figure 5) demonstrated maintenance of the reduction. There does appear to be calcification along the CC ligament at its insertion on the coracoid process, likely due to the periosteal avulsion. At six months, the patient was asymptomatic and had regained full strength and range of motion and was released to full activity. At 12 months postoperatively, the patient remained asymptomatic and had returned to playing baseball as a pitcher and football.
Stability of the AC joint is provided by both static and dynamic restraints. A cadaveric biomechanical study showed the AC capsule and ligaments primarily resist posterior translation, while the conoid ligament primarily resists anterior and superior translation of the clavicle.13 The trapezoid ligament was found to be most important when the clavicle moved towards the acromion in compression.13 The anterior deltoid originates from the clavicle, and provides dynamic stability along with the trapezius through its fascial insertion over the acromion and posterior clavicle.14 The coracoid process plays an important role in AC joint stability through the CC ligaments, and is also the site of origin for the conjoined tendon of the coracobrachialis and short head of the biceps as well as the insertion of the pectoralis minor and coracoacromial ligaments.15 The superior shoulder suspensory complex (SSSC) is a bony and soft tissue ring consisting of the acromion process, AC joint, distal clavicle, CC ligaments, coracoid process, and glenoid.16 These structures play an important biomechanical role in maintaining a stable upper extremity – axial skeletal connection.16
AC joint and distal clavicle injuries often occur with a direct blow to the shoulder on the cephalad surface of the acromion. The resultant force causes inferior displacement of the acromion in relation to the clavicle. In a child, physeal fracture occurs at the distal clavicle due to the stronger AC ligaments holding the epiphysis in place.17 As the scapula further displaces inferiorly, increased stress is placed on the CC ligaments and coracoid process. Typically, the stronger CC ligaments remain intact and cause epiphyseal separation of the coracoid process.17,18 However, in this patient, the CC ligaments avulsed from their attachment at the coracoid, and a fracture occurred through the base of the coracoid making this an unusual injury pattern.
The literature regarding treatment of injuries to the distal clavicle and surrounding SSSC in children is limited. Most agree that nondisplaced or minimally displaced injuries (Types I, II, and III) can be treated conservatively.19-21 These injuries are managed with sling immobilization followed by early rehabilitation with range of motion exercises. Management of displaced distal clavicle injuries (Types IV, V, and VI) in children remains controversial. Some recommend conservative treatment with good functional outcomes reported,3,22 however, there is a higher likelihood of developing a ‘Y’-shaped distal clavicle.17,19 While this deformity does not cause a significant functional deficit, some patients may seek excision of the bony overgrowth for discomfort or cosmesis.3,19 Therefore, some authors recommend open reduction and internal fixation for displaced injuries (Types IV, V, and VI).4,17,19 Historically, K-wire fixation was utilized with a risk of local wound complications.4,17,19 In 2013, Rashid et al.23 reported successful management of displaced distal clavicle injuries in five children with the use of an open tension band repair of the distal clavicle using an absorbable suture, similar to the technique described in this case. A 2-mm hole was drilled through the distal clavicle metaphysis in an anterior-posterior direction and a heavy absorbable suture was passed through this hole and then the epiphyseal fragment, or through the AC joint if the epiphyseal fragment was too small and tied in a figure-of-eight configuration. At a mean follow-up of 26 months (range 6 to 42) all patients reported excellent functional outcome with a Quick-DASH score of 0 and full active range of motion.23
In cases of ‘double’ or ‘triple injury’ to the SSSC, surgical treatment is often recommended.6-12 Montgomery and Loyd reported on two similar cases in 15-year-old boys with complete AC separation and an avulsion fracture at the insertion of the CC ligaments at the coracoid process.10 One patient was managed surgically with reattachment of the avulsed CC ligaments to the coracoid with non-absorbable suture, which resulted in a successful outcome and full return to sports. The other was managed conservatively in a sling for 4 weeks. At final follow-up at one year, the patient managed conservatively complained of aching pain at the AC joint with activity and was distressed by the cosmetic deformity of the high-riding clavicle.10 Kirkos et al. described a similar case in a 12-year-old boy of a completely displaced fracture of the lateral clavicle physis with rupture of the CC ligaments.12 They reported successful outcome at two years following surgical repair of the CC ligaments with non-absorbable suture and placement of K-wires to hold reduction of the distal clavicle that were removed at six weeks.12 Jettoo et al. reported a case of true AC joint dislocation and base of the coracoid fracture in a 12-year-old boy.11 This was treated with open reduction and screw fixation of the coracoid and reduction and fixation of the AC joint with threaded half pins. The threaded pins were removed at four weeks, and the patient had resumed full activities and was asymptomatic at final follow-up at nine months.11
In the previously reported cases of ‘triple injury’ to the SSSC, operative intervention to address the three sites of injury resulted in successful outcome (Table 1).6-9 The rationale for operative intervention was most often the amount of initial displacement of the distal clavicle and the fact that a displaced coracoid process fracture cannot be reduced and expected to unite with the use of any external device.6-9
In this case, given the amount of displacement of the distal clavicle and concomitant fracture of the base of the coracoid, we felt operative intervention was most appropriate to restore normal anatomy and function of the SSSC. Open reduction and internal fixation with a lag screw through the coracoid process gave a stable base for suture anchor repair of the avulsed CC ligaments. We utilized a similar suture repair technique reported by Rashid et al. to hold reduction of the distal clavicular physeal separation and repair the disrupted periosteum while avoiding wound complications associated with K-wires.23 This resulted in a successful outcome, with return to full activity and sports.
Distal clavicular physeal separation (AC ‘pseudo-dislocation’) with fracture of the coracoid process and CC ligament rupture is a rare injury. When a >100% displaced distal clavicle separation occurs, careful scrutiny of radiographs are important to identify other sites of injury to the SSSC. When ‘double’ or ‘triple injuries’ are identified, we recommend operative intervention to address all sites of injury.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}