
Influence of Season and Weather on Adult Orthopaedic Trauma Volume and Severity
Arthur E. Hess, MD, Mark S. Vrahas, MD, Suzanne M. Morrison, MPH, Amber M. Hall, MS, David Zurakowski, PhD, Michael J. Weaver, MD
The authors report no conflict of interest related to this work.
©2018 by The Orthopaedic Journal at Harvard Medical School
 PDF
PDFBACKGROUND To determine seasonal variability and influence of weather on adult orthopaedic trauma volume at two American College of Surgeons (ACS) Level I trauma centers in New England.
METHODS Adult orthopaedic injuries consisting of extremity and pelvic fractures and dislocations over a five-year period were examined for seasonal trends in both total orthopaedic volume and open fracture volume. We looked for variability dependent on weather conditions including maximum daily temperature, precipitation, and projected daylight hours.
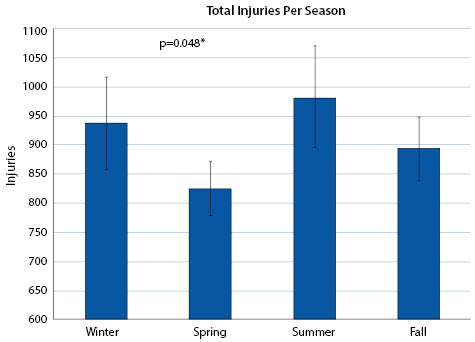
RESULTS Seasonal variation in both total volume of injuries and open fractures was observed. There was higher average volume of total injuries in the winter (937 ± 79) and summer (982 ± 87) months compared to spring (826 ± 46) and fall months (893 ± 54; p<0.001). Higher maximum daily temperatures were correlated with more injuries, with average injuries per day highest in the hottest quartile days (10.0 ± 4.6). Similarly, more open fractures occurred in the hotter quartile days. With every 5 degree rise in maximum temperature, the odds of an injury being open increased by 10%. Precipitation had no effect on total volume, but was weakly correlated with a decreased volume of open fractures (r=-0.06). Number of daylight hours had a small effect on both total volume and number of open fractures, but this correlation was also weak (r=0.113).
CONCLUSION In New England, there is seasonal variability in adult orthopaedic trauma with higher volume and open fractures occurring in the summer months. Higher ‘temperatures and longer days were predictive of higher volume of total injuries and open fractures.
LEVEL OF EVIDENCE Prognostic Level III
KEYWORDS Weather, trauma, volume, fracture, precipitation
Daily orthopaedic trauma patient presentation is highly varied; however, literature fails to comprehensively describe how weather patterns may affect this variation. Certain studies document increased trauma admissions in summer months whereas others note a higher incidence of hip fractures and traumatic falls during the winter.1-6 Literature pertaining to volume of trauma admissions consistently links hotter, dryer days with increased patient traffic; however, the connection between weather patterns and hip fracture incidence is less clear.2,7-14 Increased presentation occurs during periods of snow and ice, and more generally, severe weather warnings correspond with a 40% boost in orthopaedic trauma patient volume.15-17 While the impact of weather on orthopaedic injury volume is robustly discussed, there is a paucity of literature that examines the impact of specific weather conditions on type and volume of orthopaedic trauma injuries.
The primary purpose of this study is to evaluate the effect of season and weather on adult orthopaedic trauma volume presenting to two academic American College of Surgeons (ACS)-verified Level 1 trauma centers. Secondarily, we assessed the influence of season and weather on the severity of orthopaedic fractures using open fractures as a surrogate marker. We hypothesize that seasonal trends will demonstrate increased volume and higher severity injuries on long, dry, hot days.
We performed a retrospective review of all patients treated at two academic ACS Level I Trauma hospitals in a large New England metropolitan area from January 1, 2008 to December 31, 2012. Institutional review board (IRB) approval was obtained prior to the initiation of the study. A registry of all patients seen and treated by the Orthopaedic Trauma Service at these hospitals is maintained in a prospectively-collected database. Inclusion criteria consisted of patients over the age of 18 who had sustained fractures or dislocations treated within the abovementioned time period. Demographic and injury data was collected including patient sex, age at presentation, presentation date, mechanism of injury, side of injury, open vs. closed injury (Gustilo classification),18-19 injury description, and AO/OTA fracture classification code (if applicable). Patients were excluded if they had isolated hand, forefoot, or spine injuries, a prosthetic joint dislocation, or a pathologic fracture.
Historical daily weather conditions for the metropolitan area over the five-year period were obtained from the National Oceanic and Atmospheric Administration’s National Climatic Data Center website (www.ncdc.noaa.gov). Duration of daylight (sunrise to sunset) was obtained from United States Naval Observatory website (www.usno.navy.mil/USNO). Data obtained from these two sources included projected hours of daylight, temperature readings, weather conditions, and amount of rain/frozen precipitation.
Statistical analysis was performed in SPSS (version 21.0, SPSS Inc./IBM, Chicago, IL). Kruskal-Wallis test was performed to establish normality. Quartiles were derived for maximum daily temperature or Tmax (≤7C, 8-15C, 16-23C, and ≥24C) and projected daylight in minutes (≤610 minutes, 610-734 minutes, 735-854 minutes, ≥855minutes) to ensure even daily distribution. Furthermore, seasonality was categorized into 4 groups with 3 months per group. Seasons were defined as the following: Winter from December 1 to February 28 (29); Spring from March 1 to May 31; Summer from June 1 to August 31; Fall from September 1 to November 30. Analysis of variance (ANOVA) was used to determine significance of Tmax, daylight time, or seasonal variation for total number of injuries (volume) and open fractures. Precipitation was defined as having 2.5 millimeters or more of water equivalent precipitant, as defined by the National Weather Service, and evaluated using an independent Student t-test. Additionally, daily maximum temperature (Tmax), precipitation, and projected daylight were analyzed relative to volume and number of open fractures using Pearson correlation coefficients.
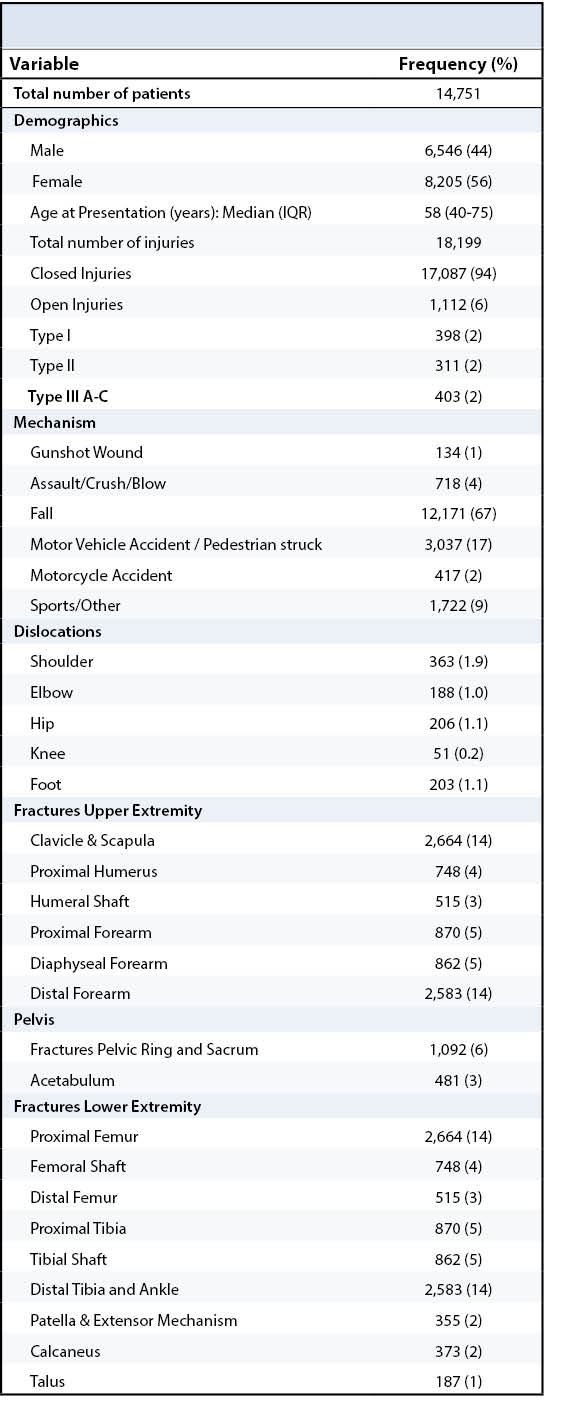
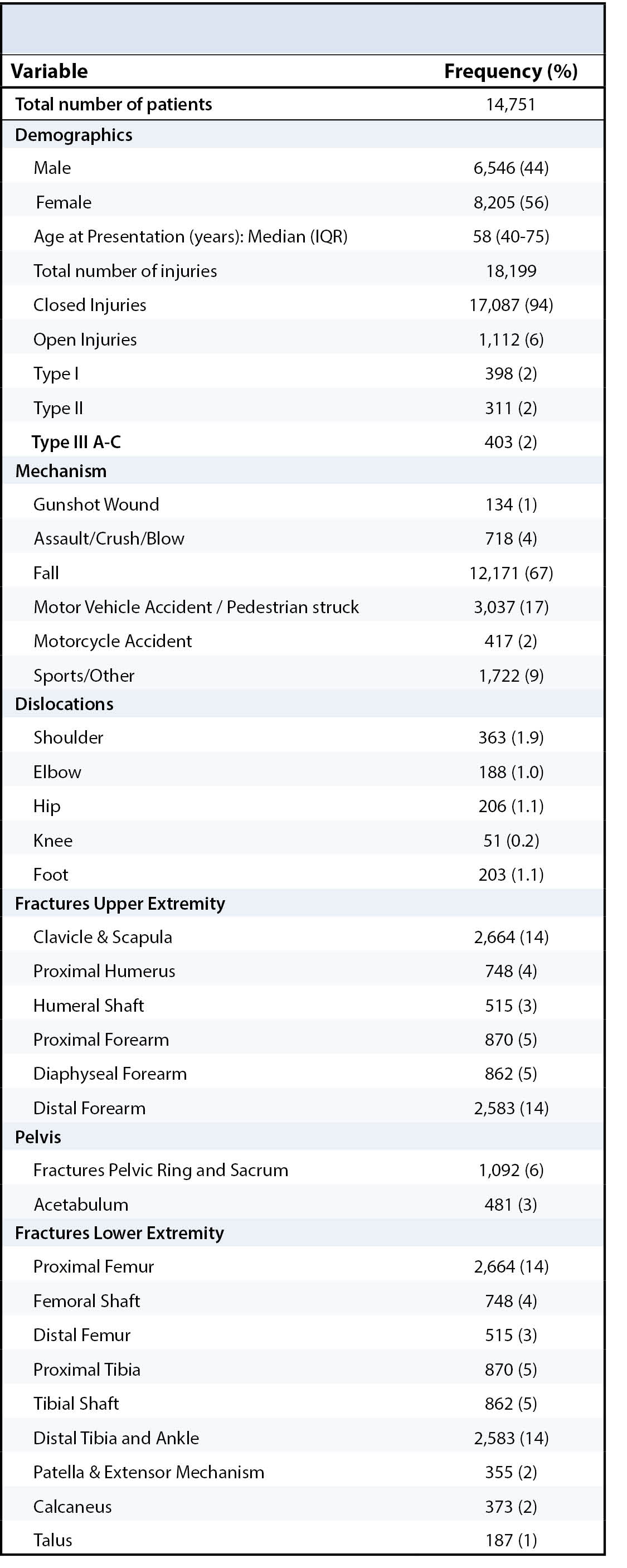
A combined total of 18,199 orthopaedic injuries were included in the dataset from a total of 14,752 patients treated over the five year period. Of these patients, 8,205 (55.6%) were female, and median age was 58 years (IQR: 40-75years). Patient demographic data and injury-specific data are presented in Table 1.
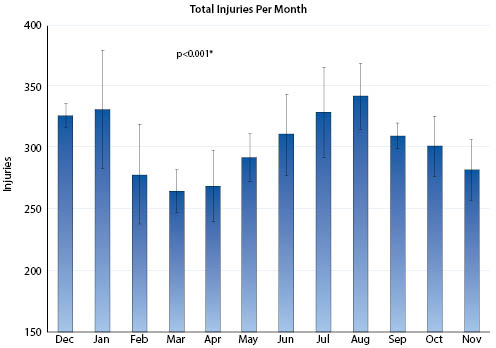
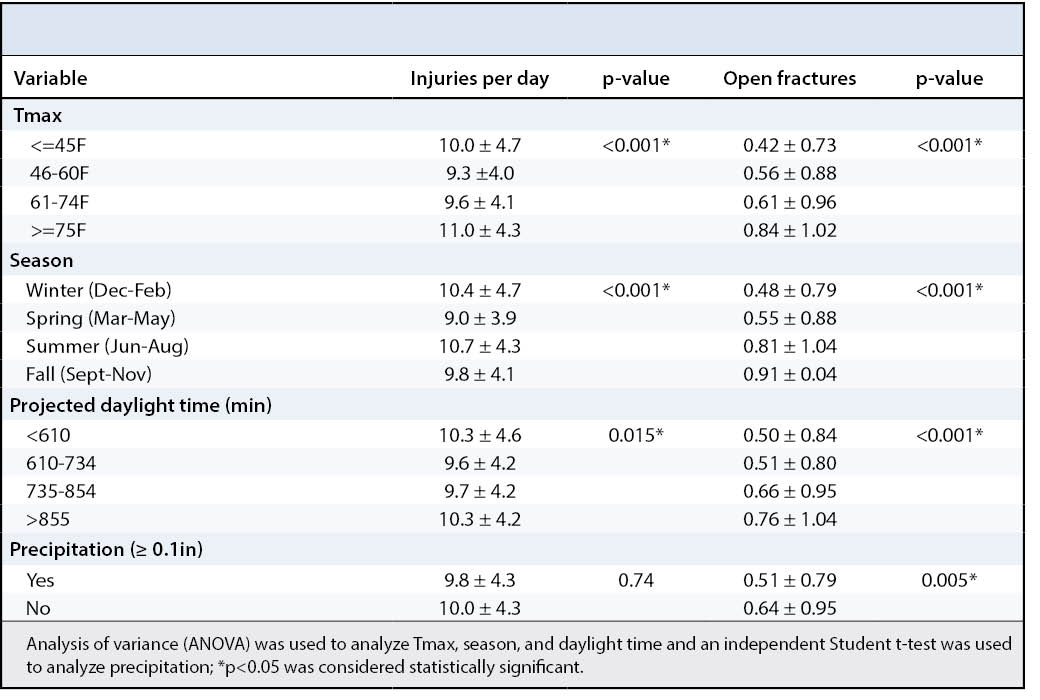
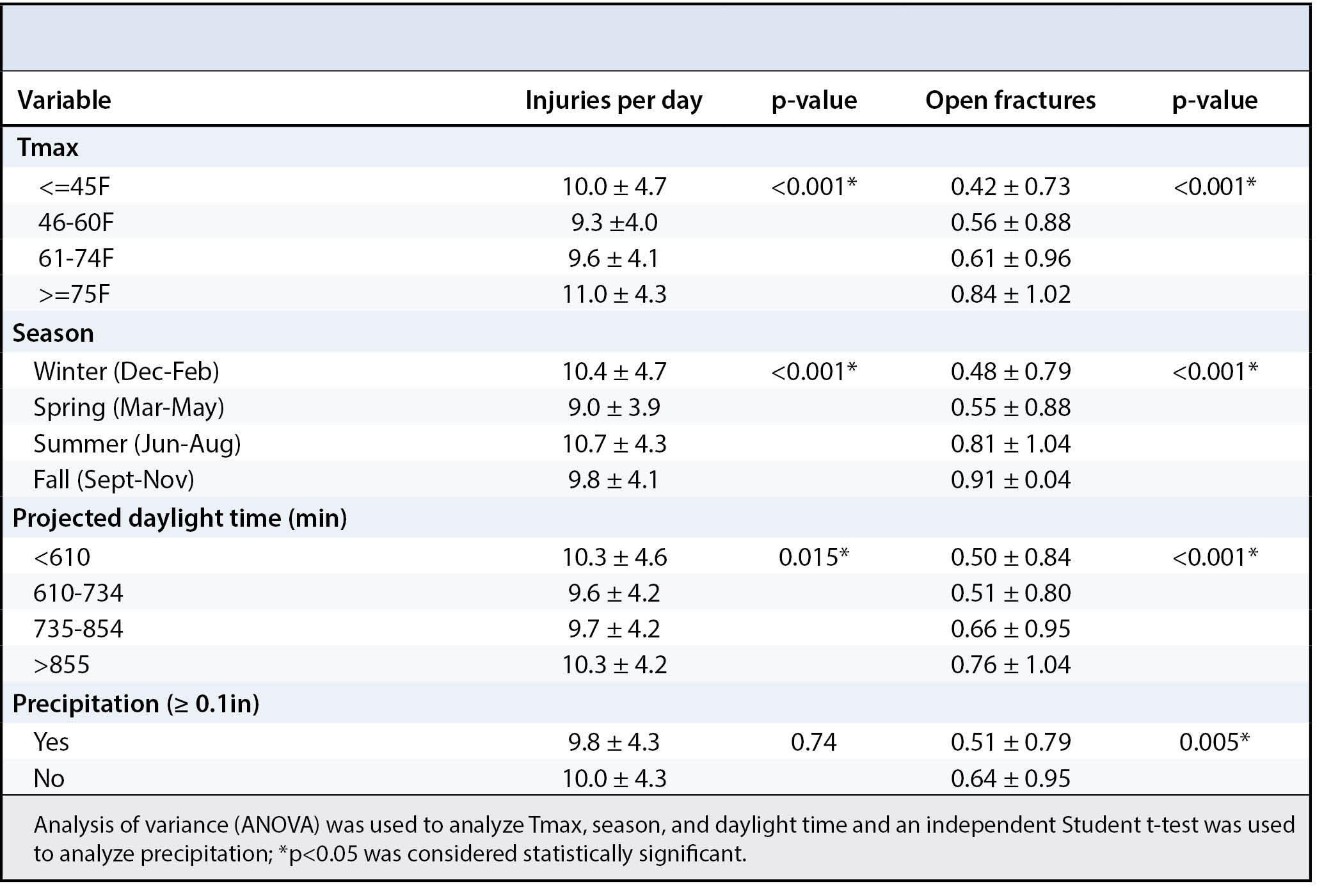
Month–to-month analysis revealed a bimodal pattern in the volume of injuries seen throughout the year, peaking during the summer (10.4 ± 4.7 injuries per day) and winter months (10.7 ± 4.3 injuries per day; p≤0.001) (Figure 1 and Figure 2). Trauma volume was related to daily maximum temperature (Tmax) in that statistically higher volumes of injuries occurred in the coldest (10.0 ± 4.7) and warmest (11 ± 4.3) quartiles compared to the moderate temperature quartiles (fall, 9.3 ± 4.0; and spring, 9.6 ± 4.1, respectively), p≤0.001 (Table 2).
Analysis of variance (ANOVA) was used to determine significance; *p < 0.05 was considered statistically significant
Analysis of variance (ANOVA) was used to determine significance; *p < 0.05 was considered statistically significant
Routine Care
The number of daylight hours was not correlated with the orthopaedic trauma volume seen (r=0.008, p=0.72). Precipitation was also not significantly associated with orthopaedic trauma volume whether treated continuously (p=0.16, r=-0.033) or as a dichotomous variable (p=0.74) (Table 2).
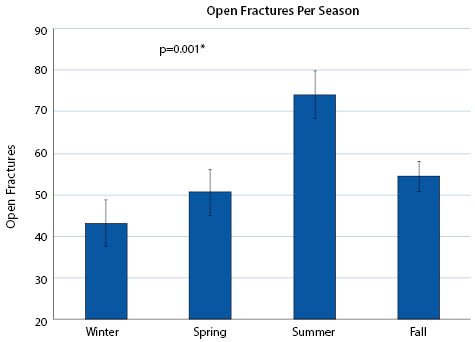
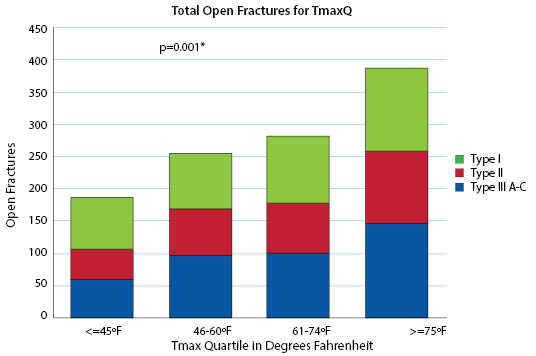
With respect to severity of injury, a significant correlation between open fractures and season was observed. More open fractures occurred in the summer compared to the winter, spring or fall (p≤0.001 for each comparison) (Figure 3). Furthermore, daily maximum-recorded temperature quartiles displayed significantly more open fractures with warmer temperatures (p≤0.001) (Figure 4). Multivariable regression analysis of open fractures and temperature revealed that with every 5 degree rise in maximum daily temperature, the odds of an injury being an open fracture rose by 10%, independent of volume for the day. The proportion of open injuries was greater in the summer months; this was demonstrated by the significantly higher percentage of open fractures among total injuries in the summer (7.5% ± 0.8) compared to the winter (4.6% ± 1.6) (p=0.003).
Analysis of variance (ANOVA) was used to determine significance; *p < 0.05 was considered statistically significant
Analysis of variance (ANOVA) was used to determine significance; *p < 0.05 was considered statistically significant
Precipitation amount was inversely related to number of open fractures continuously (p=0.008) and categorically (p≤0.005) but only demonstrated a weak effect (r=-0.06). Projected daylight was also correlated with an increase in the number of open fractures both continuously (p≤0.001) and categorically (p≤0.001), but, likewise, had a relatively weak effect (r=0.113) (Table 2).
In the present study, we assessed how total adult orthopaedic trauma volume seen at two academic ACS-designated Level 1 Trauma hospitals is affected by seasonal variation and daily weather conditions. Weather conditions chosen for this study included maximum temperature (Tmax), precipitation, and projected daylight hours. These variables were chosen as they have historically been shown to have an impact on health resource utilization including hospitalization and fracture incidence.2,7-10,25 We further examined the effects of these weather variables specifically on open fractures.
This study demonstrates significant seasonal variation in adult orthopaedic trauma volume; specifically, a bimodal distribution was seen displaying a higher volume of trauma seen in the summer and winter months compared to the spring and fall months. The summer and winter months had 12.5% more injuries than the spring and fall months. Additionally, Tmax was found to be a predictor of total volume as higher volumes were observed in the extreme temperature quartiles (≤7C degrees, and ≥24C degrees). Precipitation did not correlate with overall trauma volume. Projected daylight did correlate weakly with overall trauma volume however, the effect was minimal. This data allows for improved resource allocation to account for expected variation in trauma volume throughout the year.
Seasonal variation was also demonstrated with regard to open fractures. There were larger numbers of open fractures seen in the summer months and, to a lesser degree, winter months. In addition, the average percentage of these injuries that were open fractures increased substantially from 4.6% in the winter months to 7.5% in the summer. On hot, dry, longer days, there was a statistically significant rise in both number of open fractures and percentage of injuries that were open fractures. This likely represents an increased mechanism of injury, with patient more likely to participate in activities that put them at risk of serious injury during the warmer summer months.
This study has a number of limitations. Firstly, this study was undertaken in the Northeast United States, affecting the generalizability of our results to locations with weather dissimilar to New England. It is also possible that the trauma networks and transfer patterns within New England may effect seasonal variation in trauma beyond simple changes in weather. Future studies in multiple locales can further investigate whether it is the weather condition or the seasonality of other factors that is the true influence on orthopaedic trauma volumes. Secondly, that while large differences in volume are seen on a season to season or month to month time scale, the daily variation is so high that predicting volume based on weather variables for any given day is impossible. The effects of weather and season on orthopaedic injury volume are only useful in allocating resources on a monthly or seasonal basis.
In summary, seasonal variation of adult orthopaedic trauma volume and severity of injury was observed over a 5-year period, with higher volume and more open fractures occurring in the summer months. There was also an increase in trauma volume in the winter months. Maximum daily temperature was correlated with higher volume of injuries. Severity, as measured by open fracture volume and as a percentage was found to increase significantly on hotter, dryer and longer days. These data can be used to help justify increased resource allocation during busy months.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}