
Acute Compartment Syndrome From Peroneus Longus Rupture Treated with Fasciotomy and Peroneus Longus to Brevis Tenodesis
Janice J. He, MD and Yi-Meng Yen, MD, PhD
The authors report no conflict of interest related to this work.
©2018 by The Orthopaedic Journal at Harvard Medical School
 PDF
PDFThis case demonstrates a late presentation of compartment syndrome due to peroneus longus muscle rupture. This case is unusual because of the complete loss of the peroneus longus muscle belly which was subsequently treated with longus to brevis tenodesis and resulted in a return of function. This case highlights the necessity of being vigilant when assess patients with lateral calf pain.
LEVEL OF EVIDENCE Case Report Level V
KEYWORDS Muscle tear
Compartment syndrome is an elevated pressure within a fascial compartment causing muscle ischemia due to decreased perfusion.1 Timely diagnosis and fasciotomy is critical, as a delay in treatment can result in nerve dysfunction and muscle necrosis which can lead to contractures, significant loss of function of the limb, and even amputation.2 Acute compartment syndrome is most commonly caused by trauma and is most often associated with long bone fractures and blunt force injury. However, there can be other atypical causes of compartment syndrome such a chronic exertional compartment syndrome or a vascular insult.3,4 The anterior compartment is most frequently affected in acute compartment syndrome of the lower extremity. However, isolated acute lateral compartment syndrome has been reported. In these cases, the cause is rupture or avulsion of the peroneus longus muscle, most frequently reported after non-contact ankle injury in football players.5-11 In this case report, we discuss a football player who developed isolated lateral compartment syndrome nine days after suffering a peroneus longus rupture from a non-contact sports injury. This case is unique in that the patient lost the entire peroneus longus muscle belly, however function was preserved by performing a peroneus longus−to−brevis tenodesis.
An 18 year-old male high school quarterback suffered a twisting injury during a football game. At that time, he reported that he felt lateral leg pain after planting his foot, inverting his ankle and attempting to jump. He resumed play and did not immediately seek medical attention. He iced his calf and received daily massages for symptom relief. He played in his next high school game. However, nine days after the initial injury, he presented to an outside hospital emergency room with increasing pain, as well as numbness and paresthesias in his deep and superficial peroneal distributions.
His past medical and surgical history were unremarkable. He took no medications. On examination, he was in moderate distress. He had a tense lateral compartment on palpation. He had significant pain with passive range inversion and eversion of his ankle. He had diminished sensation in his deep peroneal and superficial peroneal nerve distributions. Sensation was intact in the tibial, saphenous and sural distributions. He had palpable dorsalis pedis and posterior tibialis pulses. Plain radiographs of his ankle were negative for acute fracture. Compartment pressures were not obtained, but his clinical presentation was consistent with evolving acute compartment syndrome of his leg.
He was taken emergently to the operating room for fasciotomy, and the anterior and lateral compartments of the leg were released. It was noted during this initial procedure that there was significant hematoma in his lateral compartment which was evacuated. A large tear in the muscle belly of the peroneus longus was noted, the muscle appeared dusky and gray, and an attempt was made to repair this muscle. A wound vacuum dressing was placed over the leg wound and a large vessel loop utilizing the “Roman sandal” technique was applied under tension. The patient was transferred to a tertiary care center on post−operative day three.
On transfer, the patient was well appearing. His sensation was fully intact in his leg and foot. He had palpable dorsalis pedis and posterior tibialis pulses. He was able to actively dorsiflex, plantarflex, evert and invert at his ankle. He was brought back to the operating room on post-operative day four for a wound exploration. The peroneus longus muscle belly was significantly darker than the surrounding muscle (Figure 1). A nerve stimulator was placed on the peroneus brevis, which was completely viable. However, the peroneus longus did not respond to electrical stimulation. The muscle belly was placed back loosely into the wound and a new vacuum dressing applied without the use of a “Roman sandal” vessel loop with a plan for a third operative assessment to reassess for peroneus longus survivability.

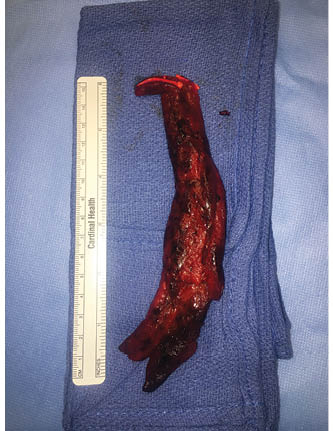
On post-operative day seven, the patient was taken back to the operating room. The peroneus longus appeared black and necrotic (Figure 2). The muscle belly did not contract to electrical stimulation or bleed when a needle was inserted into it. The decision was made to debride the non-viable muscle, which consisted of the majority of the peroneus longus muscle belly (Figure 3). The original fasciotomy incision was extended distally to identify the peroneus brevis tendon. While holding the foot in neutral, the remaining distal peroneus longus tendon was then tenodesed to the peroneus brevis. The skin was then closed and the patient placed into a tall Controlled Ankle Movement (CAM) boot to prevent equinus contracture. Post-operatively, the patient was permitted to weight bear as tolerated. The immediate post-operative course was uneventful and the patient was discharged on post-operative day one from his last surgery.

The peroneals are the primary evertors of the foot with the longus being stronger than the brevis.13 Additionally, the peroneals assist in plantarflexion and serve as dynamic stabilizers of the lateral ankle. The peroneus longus, which travels across the plantar aspect of the foot to insert on the first ray also serves to support the transverse arch of the foot. A tear of this muscle or tendon can occur with an acute forceful inversion injury. An acute rupture of the peroneus longus muscle belly from this mechanism is very rare with only case reports in the literature.5-11,14 The presumption is that the hematoma formation at the proximal origin likely causes an isolated lateral compartment syndrome. All patients reported in the literature were all treated with fasciotomy although usually with minimal to no muscle debridement and recovered with good short term return of muscle function.
In this case, the patient presented in a delayed fashion and thus there was delay to fasciotomy, resulting in the need for extensive debridement of the entire peroneus longus muscle belly. In contrast, in the previously reported case reports, the patient presented within the first 48 hours from injury, the muscle was contractile with stimulation, and was retained and healed over time. The significant delay in presentation and use of the Roman sandal technique under tension after fasciotomy (rather than applying this loosely) may have contributed to the continued necrosis of the muscle belly. Significant debridement of the peroneus longus muscle has been reported by Merriman et al. and Moyer et al., but some muscle tissue was able to be retained.10,14 In our patient, the entire muscle belly was debrided with only the tendon remaining. The remaining peroneus longus tendon was tenodesed to the peroneus brevis to help mitigate peroneal weakness and lateral ankle instability. Redfern et al. have described this technique in their case series of patients with chronic peroneal injury with significant improvement of function.13 Post-operatively, the patient had no pain, no instability, and had 5/5 strength in foot eversion when seen at his last follow-up at four months.
Although acute compartment syndrome after peroneal muscle injury is quite rare, a high index of suspicion and a thorough physical examination is critical for prompt diagnosis. This diagnosis should be considered in a patient who has sustained a lateral ankle injury and who reports lateral calf pain.



{kind=link}
{kind=link}
{kind=link}