|
|
|
| Click here to visit our web site |
|
Management of posterior cruciate ligament (PCL) injuries continues to be a controversial topic in sports medicine. Good short-term results have been reported with non-operative treatment, but longer-term studies suggest that late knee arthrosis develops in 36-88% of patients with untreated PCL insufficiency. (1,7) Appropriate operative treatment for PCL injuries remains unclear. Various methods of PCL repair and reconstruction have met with limited clinical success, and knee arthrosis has been reported in 20% to 60% of patients even after operative treatment. (3,6,9) Thus, PCL reconstruction continues to be the focus of research efforts. Experimentally, with the appropriate selection of graft tunnel location and initial graft tension, both single- and double-bundle PCL reconstruction can restore in vitro anteriorposterior stability. (2,10) However, all in vitro biomechanical studies to date have focused on evaluation of PCL reconstruction by measuring anterior-posterior laxity under sagittal plane posterior drawer testing. The effects of surgical reconstruction on the three-dimensional kinematics of the knee remain unclear, especially with regard to rotational kinematics. Few data have been reported on the three-dimensional kinematic behavior of the knee after PCL reconstruction, under functional loading conditions. Our goal in this study was to determine whether in vitro PCL reconstruction could restore not only posterior tibial translation but also knee joint rotations under simulated muscle loads. Using the robotic testing system, a series of human cadaveric knee specimens were tested. A joint coordinate system was established with the knee center defined as the center point of the transepicondylar line and the transepicondylar axis as the flexion/extension axis. The following testing protocol was applied: the passive flexion/extension path was first determined, and then the kinematic behavior (displacements and rotations) was recorded in response to a posterior drawer load of 130N, a quadriceps load (400N), and a combined quadriceps and hamstrings load (400/200N), at selected flexion angles. This protocol was applied to each knee sequentially in intact, PCL resected, and PCL reconstructed states. Reconstruction of the anterolateral bundle of the PCL was performed using an Achilles tendon allograft. (8) The bone block was fixed on the femoral side using an outside-in interference screw. The tibial tunnel was drilled slightly lateral to midline, 1cm below the articular surface. The posterior capsule was carefully elevated distally off a 2cm area at the tibial tunnel site to facilitate passage of the graft. Tibial fixation was performed with the knee at 90° flexion under a 130N anterior drawer load, using a soft-tissue interference screw augmented with a cortical spiked ligament washer. In this fashion, each specimen was tested sequentially with the PCL intact, resected and reconstructed, with the serial application of external loads and measurement of knee kinematics. All displacements and rotations were reported with respect to the original, intact knee passive path. Our results demonstrate that, under posterior drawer loading, posterior tibial translation was greater in PCL resected knees than in intact knees at all flexion angles. PCL reconstruction reconstruction significantly reduced posterior tibial translation at all flexion angles when compared to PCL resected knees, to levels not significantly different than those observed in intact knees. These results are in agreement with those reported in the literature. (2,4,5)
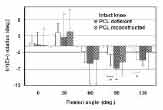
Under both isolated quadriceps and combined quadriceps and hamstring loading conditions, posterior tibial displacement was again greater in PCL resected than in intact knees at high flexion angles. However, the PCL reconstructed knee did not exhibit consistently reduced posterior displacement under simulated muscle loading (Figure 6). This phenomenon demonstrates that after PCL reconstruction, knee kinematics may be restored under posterior tibial drawer loading, but are not consistently restored under muscle loading. Under simulated muscle loading conditions, increased tibial external rotation was observed at high flexion angles (Figure 7); this again was not consistently reduced by PCL reconstruction. We observed that there was significant variability in rotational knee kinematics after PCL reconstruction, particularly at increased flexion angles. We believe that the location of the tibial tunnel, and therefore the point of graft force application, may play an important role in the rotational kinematics of the reconstructed knee. The precise placement of the tibial tunnel has not been stressed in the current surgical treatment of PCL deficiency. 8 Further study of the effects of tibial tunnel placement on rotational kinematics of the PCL reconstructed knee is warranted.
Our results demonstrate that PCL reconstruction using an Achilles tendon graft restores normal posterior tibial translation when the knee is examined under posterior drawer loading, but does not completely correct the posterior translation and external rotation of the tibia resulting from PCL deficiency, when assessed under simulated muscle loading. This implies that posterior drawer testing of the PCL reconstructed knee does not accurately evaluate the complex kinematic responses of the knee under simulated physiologic loading conditions. Our ability to successfully reconstruct the PCL and restore knee joint kinematics under physiological loading conditions remains limited. We are currently investigating the influence of the tibial tunnel location on rotational kinematics of the PCL reconstructed knee. In addition, we hope to further elucidate the relationship between kinematics of the PCL reconstructed knee and joint contact pressures. Ultimately, this will help us to predict if PCL reconstruction is successful in preventing the long-term arthrosis of the knee. By understanding the individual benefits and shortcomings of various reconstructive techniques, it is hoped that an optimum PCL reconstruction technique will be developed in order to minimize the onset of degenerative arthritis. ACKNOWLEDGEMENTS This study was supported by grants from the Orthopaedic Education and Research Foundation (OREF), the National Football League (NFL) Charity Foundation and a Whitaker Foundation Graduate Fellowship.
|
|
Print Manuscript • View References • Download PDF version • Close window |