
Surgeon Experience in Transitioning from Transtibial to Anteromedial Portal Drilling in Anterior Cruciate Ligament Reconstruction
Randy M. Cohn, MD, Guillaume D. Dumont, MD, Amun Makani, MD, Sean M. Hazzard PA-C, Peter D. Asnis, MD
The authors report no conflict of interest related to this work.
©2016 by The Orthopaedic Journal at Harvard Medical School
 PDF
PDFPURPOSE Recent evidence suggests that anterior cruciate ligament reconstruction performed with an anteromedial (AM) portal drilling technique may better recreate the native anatomy of the femoral footprint than transtibial drilling, potentially leading to improved knee kinematics and better clinical outcomes. The purpose of this study is to describe the operative experience of a single surgeon in transitioning from transtibial to anteromedial portal drilling in ACL reconstruction. We hypothesized that, with meticulous technique, a transition to AM portal drilling can occur without an increase in intra-operative complications and with only a slight increase in operative time.
METHODS From January 2013 to December 2013, 47 patients underwent allograft ACL reconstruction by the senior author, 29 with a transtibial technique and 18 with anteromedial portal drilling. At the conclusion of the study period, all patient charts and operative reports were reviewed to assess surgical differences and intra-operative complications between the two groups.
RESULTS There were no differences between the transtibial and anteromedial groups in patient demographics or associated procedures performed. ACL reconstruction with anteromedial portal drilling had a significantly longer tourniquet time than the transtibial group (34 +/- 5 minutes versus 29 +/- 7 minutes, p = 0.015). There was a significantly increased incidence of bioabsorbable screw breakage in the anteromedial group (p=0.011), resulting in a switch to titanium interference screws in anteromedial portal ACL reconstruction. There were no further complications with interference screw placement after switching to titanium screws. There was no difference between transtibial and anteromedial portal techniques in posterior wall blowout or other intra-operative complications.
CONCLUSION Surgeons who perform ACL reconstruction with a transtibial technique can expect a slight, although significant, increase in tourniquet time while transitioning to an anteromedial portal technique. Surgeons should consider using titanium interference screw fixation while transitioning to an anteromedial portal technique to avoid femoral screw breakage during insertion of bioabsorbable interference screws.
Anterior cruciate ligament (ACL) reconstruction is one of the most commonly performed orthopaedic procedures in the United States.1 In recent decades, a transtibial technique (TT) had been advocated in order to reduce the operative time and surgical trauma associated with a two-incision technique.2-3 However, evidence is mounting that ACL reconstruction performed with TT drilling technique may not consistently and anatomically replicate the native ACL femoral footprint.4-8 As a result, knee kinematics after ACL reconstruction with a TT technique may fail to replicate that of the native knee.3,9-10 Moreover, non-anatomic graft position has been implicated as a cause of graft failure in many series.11-14
As a result, many surgeons have advocated an anteromedial (AM) portal drilling technique in order to yield a more anatomic ACL femoral footprint, recreate the obliquity of the native ACL, and allow for more anatomic placement of the tibial tunnel by uncoupling femoral and tibial drilling.15-21 Recent clinical data have suggested that AM portal ACL reconstruction may result in improved clinical outcomes with increased knee stability, range of motion, and decreased odds of repeat (ipsilateral) knee surgery.22-23
While biomechanical and clinical data may encourage surgeons to switch to an AM drilling technique, there are few studies to guide surgeons in the operating room while changing techniques.20-21 The purpose of this study is to describe the experience of a single sports medicine fellowship-trained surgeon, performing greater than 100 ACL reconstructions annually, while transitioning from TT to AM technique for ACL reconstruction. We hypothesized that, with meticulous technique, a transition to AM portal drilling can occur without an increase in intra-operative complications and with only a slight increase in operative time.
Prior to the study period, the senior author performed over 500 ACL reconstructions over a five-year period using a TT femoral drilling technique. From January 2013 to December 2013, the senior author began to transition to an anteromedial portal drilling technique. During the study period, 145 patients underwent ACL reconstruction, 96 with autograft and 49 with allograft. During the transition period, the senior author performed all autograft ACL reconstructions with a standard TT technique. ACL reconstructions with allograft were performed with TT or AM portal techniques, chosen in a non-random fashion based on surgeon preference. Of the 49 allograft ACL reconstructions, two were excluded from the study because of concomitant procedures performed during the same anesthetic. The remaining 47 allograft ACL reconstructions represent the study population. 29 operations were performed with a TT drilling technique and 18 were performed with an AM portal drilling technique.
Operative Technique
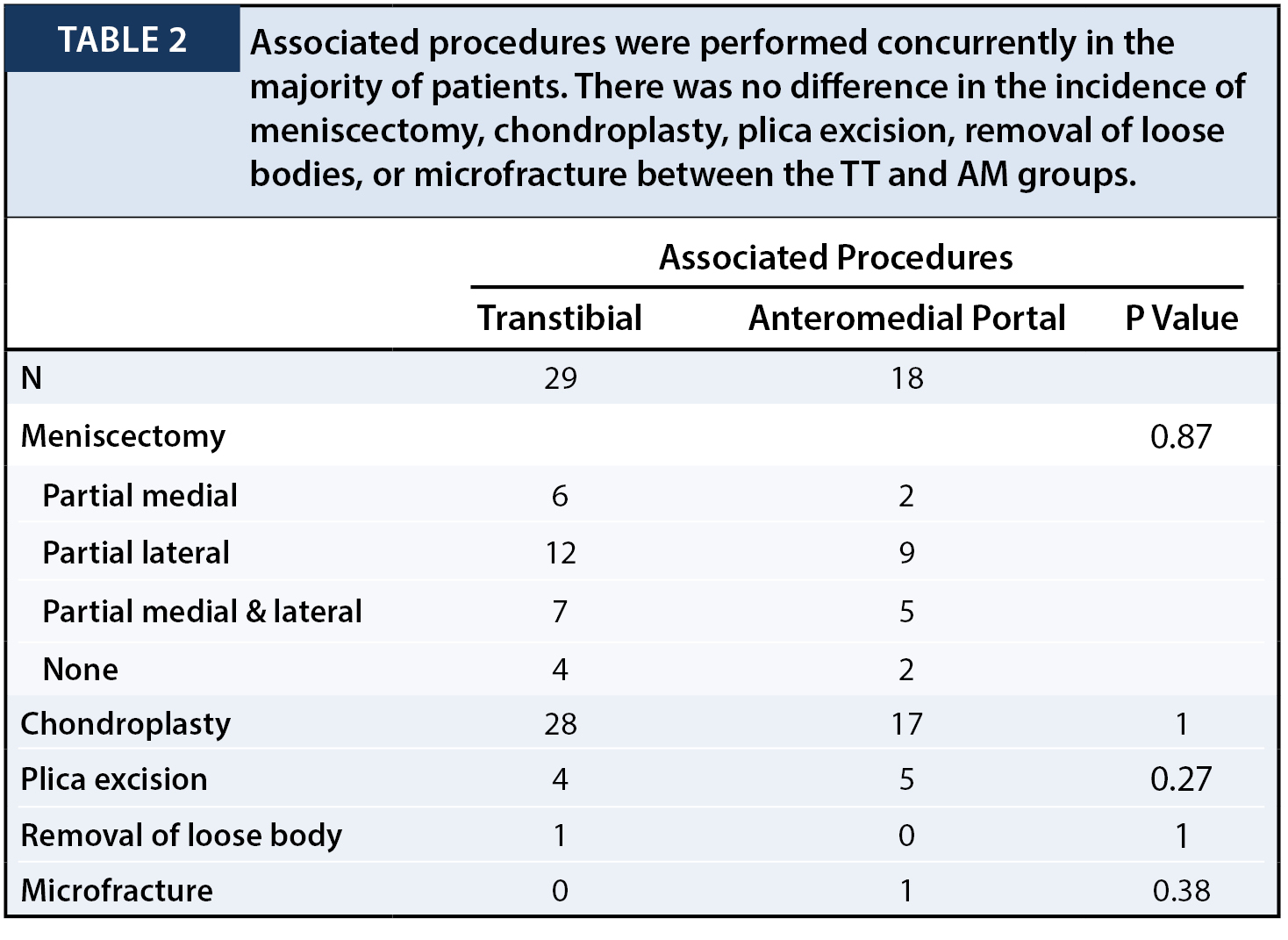
In all cases, a standard diagnostic arthroscopy was performed along with associated arthroscopic procedures, including partial meniscectomy, chondroplasty, plica excision, and removal of loose bodies, prior to insufflation of the tourniquet. The tourniquet was subsequently inflated after debridement of the ACL stump and prior to beginning the creation of the bone tunnels. The tourniquet was deflated after insertion of the femoral and tibial interference screws and prior to wound closure.
TT ACL reconstruction was performed using patellar tendon allograft in all cases. Grafts were prepared with bone plugs designed to pass easily through a 10-millimeter tunnel. The patellar bone plug was cut to 30 millimeters in length and passed into the femoral tunnel. Femoral tunnels were drilled with a 10-millimeter acorn reamer to a depth of 31 millimeters. A bioabsorbable interference screw (DePuy Mitek Milagro, Raynham, MA or Arthrex BioComposite, Naples, FL) was used for femoral fixation.
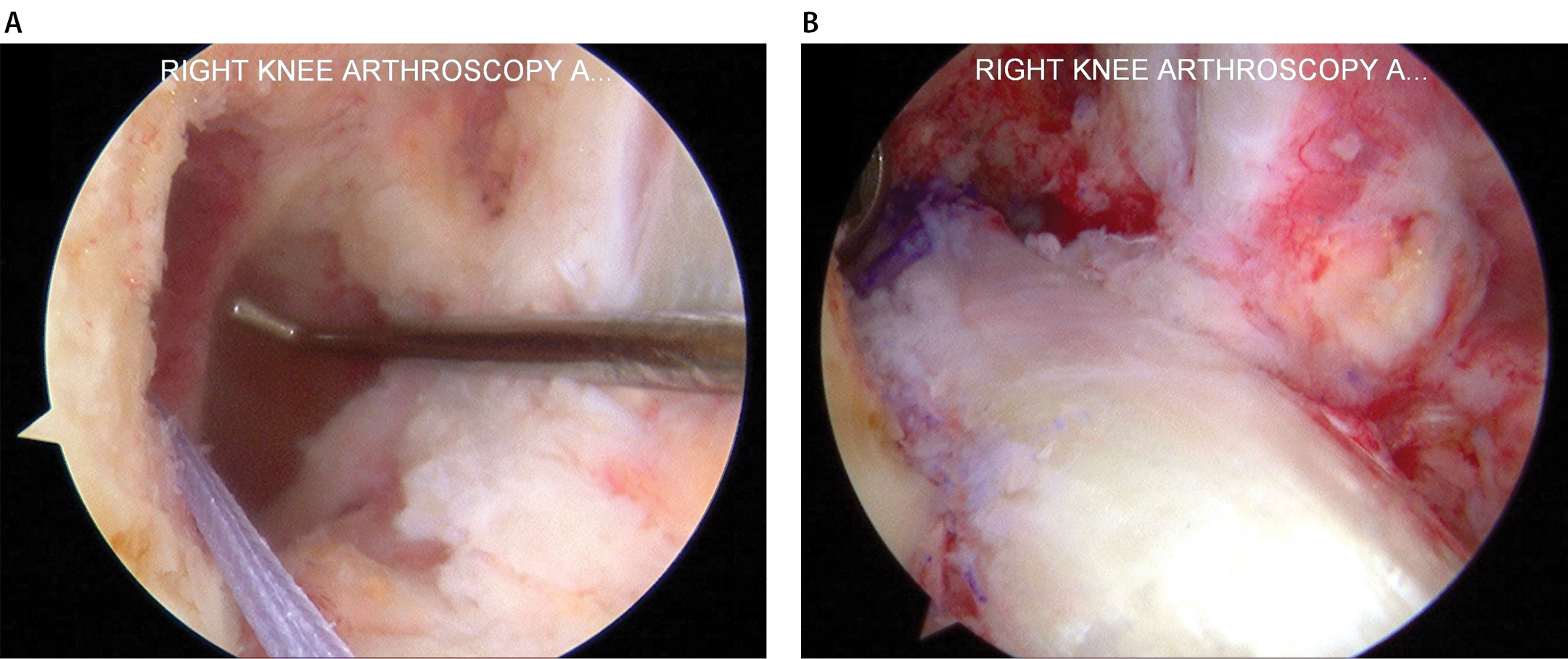
AM ACL reconstructions were performed using patellar tendon allograft, with the exception of one Achilles allograft that was used to avoid a graft length mismatch. Grafts were prepared with bone plugs fashioned to easily pass through a 10-millimeter tunnel. The femoral bone plug was cut to 22 to 23 millimeters in length and a 10-millimeter femoral tunnel was drilled to a depth of 23 to 24 millimeters (Figure 1A). Femoral tunnel drilling was performed in 105 degrees of knee hyperflexion using flexible reamers (Stryker VersiTomic, Kalamazoo, MI). Bioabsorbable interference screws (Arthrex BioComposite, Naples, FL) were used for femoral fixation initially. Titanium interference screws (Stryker Universal, Kalamazoo, MI) were used in subsequent cases secondary to screw breakage (Figure 1B).
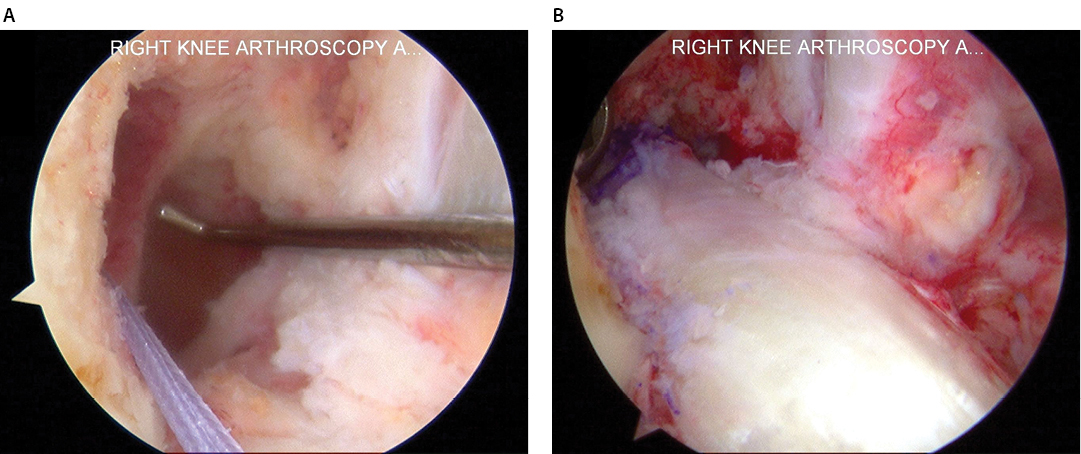
Right knee of a 51 year old female (A) A passing suture is visible in the femoral tunnel. (B) The patellar tendon allograft has been fixed with a titanium interference screw.
Statistical Analysis
Following the study period, and after approval by the institutional review board, all allograft ACL reconstructions were reviewed retrospectively to assess for differences between the TT and AM techniques, including operative time and surgical complications. Comparisons between groups on normally distributed data were done using a Student’s t-test. Comparisons of two or more groups of ordinal variables were done using contingency table analysis with chi-square or the Fisher exact probability test.
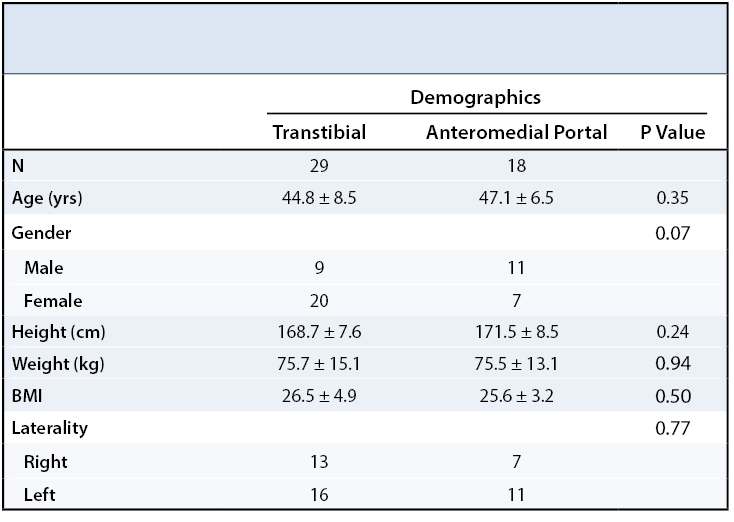
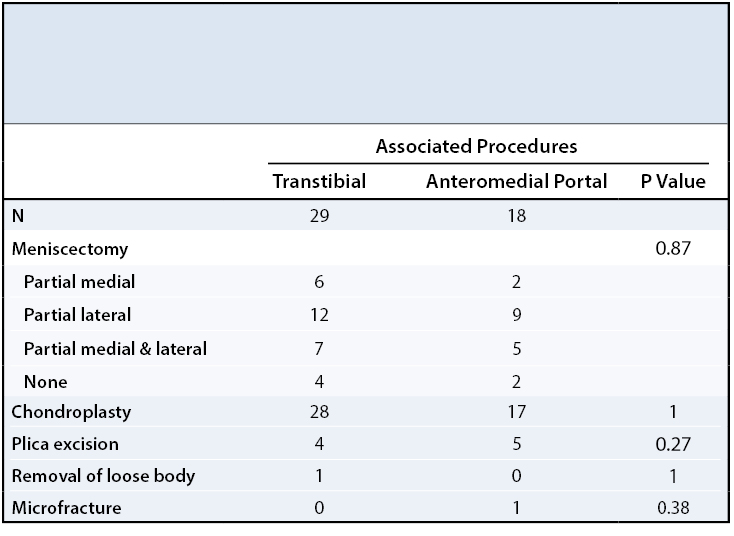
There were no differences in demographic data between the TT and AM groups, including age, gender, height, weight, BMI, and laterality of ACL reconstruction (Table 1). There was no difference in the distribution of associated procedures performed with ACL reconstruction (Table 2).
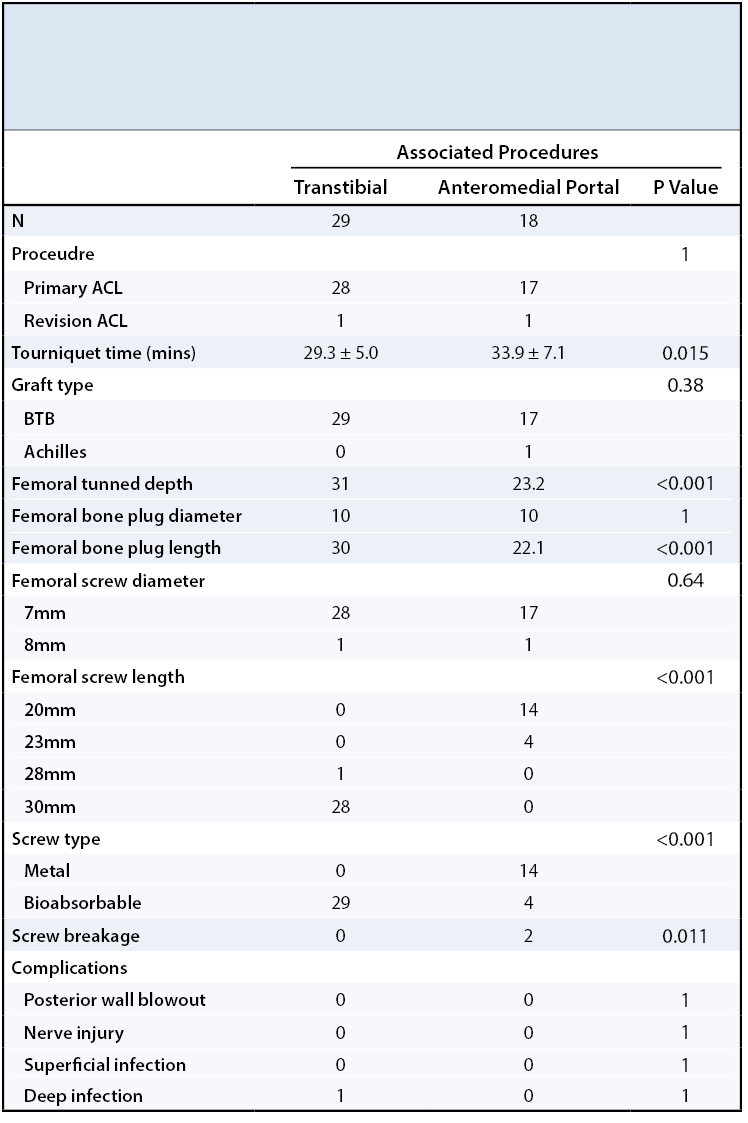
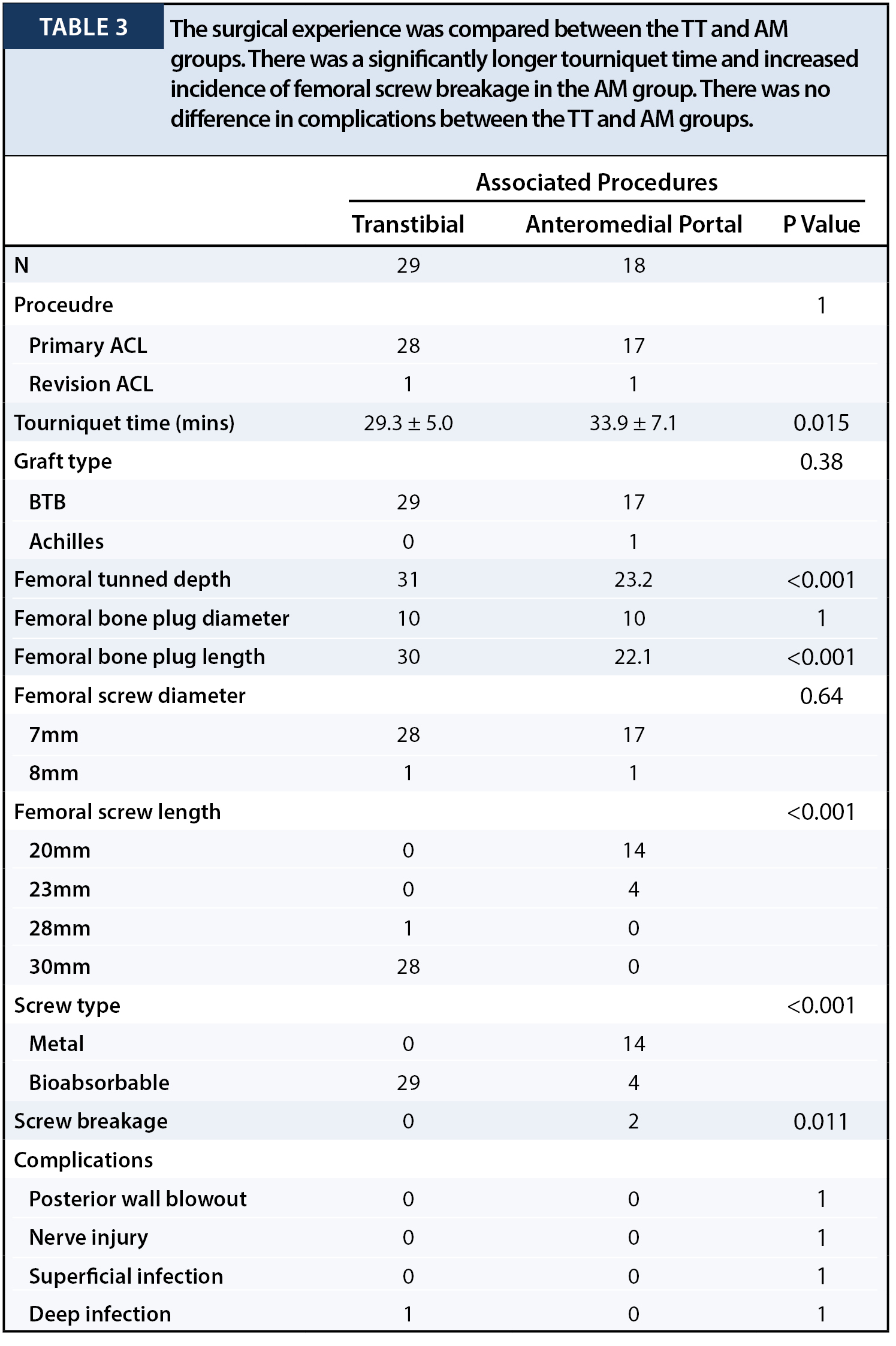
Tourniquet time was significantly longer in the AM group (p=0.015). In the TT group, average tourniquet time was 29 minutes (standard deviation (SD) 5 minutes, range 19-42 minutes), compared to 34 minutes for the AM group (SD 7 minutes, range 23-47 minutes). There were no cases of breakage of the bioabsorbable femoral interference screw in any of the 29 cases in the TT group. In the AM group, the bioabsorbable femoral interference screw broke during screw insertion in two of the four cases in which a bioabsorbable screw was used (p=0.011). In the other 14 cases in the AM group, a titanium interference screw was inserted without issue. There were no incidences of posterior wall blow out or other intra-operative complications. Surgical variables under study are found in Table 3.
Given the current biomechanical and clinical data regarding the benefits of AM drilling in ACL reconstruction, it is likely that many surgeons have considered switching from a TT technique to AM portal drilling. Many biomechanical studies have discussed the superiority of AM drilling in recreating the anatomy of the femoral footprint.2,4-6,16 Additionally, clinical studies have suggested superior outcomes and decreased odds of repeat ipsilateral knee surgery after ACL reconstruction with AM versus TT techniques.23-24 However, studies designed to help the individual surgeon switch techniques for ACL reconstruction are limited.20-21
Several authors have previously evaluated differences in femoral tunnel length and graft obliquity between AM and TT techniques.18-19,25 Chang et al. evaluated 55 TT and 50 AM ACL reconstructions with hamstring autograft to identify factors associated with tunnel length.18 Femoral tunnel length was significantly shorter in the AM group (34.2 versus 43.3 mm). Twenty-six percent of knees in the AM group and two percent in the TT group had a femoral tunnel length less than 30 mm. The authors found that a more oblique femoral tunnel and a narrower mediolateral width of the distal femur were associated with a shorter tunnel length. In our study, all TT ACL reconstructions were drilled to a depth of 31 mm and all AM femoral tunnels were drilled to a depth of 23 to 24 mm without violating the lateral femoral cortex. This difference in femoral tunnel depth is important to recognize when making the transition from TT to AM portal drilling.
Ilahi et al. reviewed 115 ACL reconstructions, 35 with TT femoral drilling and 80 with accessory AM portal drilling.25 Graft selection included hamstring autograft, patellar tendon autograft, and patellar tendon allograft, with suspensory fixation used on all grafts. Average femoral tunnel length was again significantly shorter in the AM group (35.6 mm versus 40.7 mm). The authors found that the statistical likelihood of having a femoral tunnel less than 25 mm in length with AM drilling is 0.47 percent for female patients and 0.1 percent for male patients. This finding is consistent with our study, as none of the 47 patients had a femoral tunnel less than 25 mm.
The use of bioabsorbable and metallic interference screw fixation in ACL reconstruction has been evaluated by several authors.26-28 A randomized controlled study of patellar tendon autograft ACL reconstructions performed with bioabsorbable and titanium interference screws found no difference in range of motion, knee effusions, instability episodes, or KT-1000 side-to side differences at one and two years follow-up.26 Radiographic analysis showed no evidence of osteolysis or difference in tunnel widening between the groups. The authors reported that no bioabsorbable interference screw broke during screw insertion, however they did not comment on the technique of femoral tunnel drilling used. A recent meta-analysis concluded that there was no difference in knee stability or function after ACL reconstruction with metal or bioabsorbable implants; however, the incidence of knee joint effusions was higher with bioabsorbable implants.27 The authors did not comment on the incidence of screw breakage in the bioabsorbable group.
Screw breakage with bioabsorbable femoral interference screws has been previously reported.28-30 In a study by Barber et al., bioabsorbable interference screw breakage occurred in six of 85 cases (7.1 percent) during femoral screw insertion.28 Twelve of 204 (5.9 percent) bioabsorbable femoral screws broke during insertion in the study by McGuire et al., without any adverse events or need for additional fixation besides replacement of the interference screw.30 In our study, no bioabsorbable screw breakage occurred in 29 cases with TT drilling. However, with AM portal drilling, breakage of the bioabsorbable screw occurred in two of the four cases where bioabsorbable screws were used, resulting in a switch to titanium interference screws for subsequent AM portal ACL reconstructions. The increased incidence of screw breakage with AM portal drilling in our study is possibly related to the use of flexible reamers and the subsequent creation of slightly curved femoral tunnels, compared to the straight tunnels created with TT technique or an AM technique with use of rigid reamers. Surgeons transitioning from TT to AM techniques should be aware of this factor when choosing implants for femoral fixation, as well as during screw insertion.
This study is a retrospective review of a single surgeon’s experience during the first year of transitioning from TT to AM portal drilling in ACL reconstruction. During this transition period, there were no major complications related to the change in technique used. On average, the tourniquet time with AM portal drilling was five minutes longer than TT drilling in the study population. This difference is likely due to the surgeon adjusting to a new technique, and might be expected to decrease over time with experience. Further research should focus on analyzing surgical time and complications with increased experience of AM portal drilling, as well as analyzing radiographic and clinical outcomes between the AM and TT groups.
There are several limitations to the current study. All ACL reconstructions were performed by a single surgeon using patellar tendon allograft in most cases with interference screw fixation of the femoral bone plug. Thus, the results of this study may not be generalizable to ACL reconstructions with autograft, soft tissue grafts, or with different techniques for femoral fixation. The experience of the senior author may also not be generalizable to other surgeons with varying clinical volume, training, and years in practice. Additionally, there is no radiographic or clinical follow-up on the patients in this study. Thus, we are unable to comment on the tunnel position or the clinical outcomes between the AM and TT groups. Additionally, there are a small number of patients in each group of this study. However, this represents the senior author’s experience during the first year of transitioning from TT to AM drilling, and is thus relevant to other orthopaedic surgeons who are considering changing techniques.
Surgeons who perform ACL reconstruction with a TT technique may experience a slight increase in tourniquet time while transitioning to an AM drilling technique. Surgeons should consider using titanium interference screw fixation while transitioning to AM portal techniques to avoid femoral screw breakage during insertion of bioabsorbable interference screws. With meticulous technique, the experienced ACL surgeon can expect to transition from TT drilling to AM portal technique without an increase in intra-operative complications.






{kind=link}
{kind=link}
{kind=link}
{kind=link}