
Spinopelvic Mobility as it Relates to Total Hip Arthroplasty Cup Positioning: A Case Report and Review of the Literature
Alexander M. Crawford, MD, Patrick K. Cronin, MD, Jeffrey K. Lange, MD, James D. Kang, MD
The authors report no conflict of interest related to this work.
©2020 by The Orthopaedic Journal at Harvard Medical School
 PDF
PDFHip-spine syndrome occurs when arthroses of the hip and spine coexist. Hip-spine syndrome can result in abnormal spinopelvic mobility, which is becoming increasingly recognized as a cause of dislocation following total hip arthroplasty (THA). The purpose of this article is to summarize the current understanding of normal and abnormal spinopelvic mobility as it relates to THA component positioning and to provide actionable recommendations to prevent spinopelvic mobility-related dislocations. In so doing, we also provide a recommended workup and case-example of a patient with abnormal spinopelvic mobility.
LEVEL OF EVIDENCE Level V Narrative Review
KEYWORDS Spinopelvic mobility, hip-spine syndrome, fixed sagittal plane imbalance, total hip arthroplasty
Dislocation following total hip arthroplasty (THA) causes significant morbidity for patients, and accounts for approximately 17% of all revision hip replacement surgeries.1 THA instability can have multiple causes, including component malposition, soft tissue imbalance, impingement, and late wear.2 Acetabular component positioning has been one major consideration historically for optimizing construct stability. The classic ‘safe zone’ for cup position described by Lewinneck et al. included a range of cup position at 40 ± 10 degrees of abduction and 15 ± 10 degrees of anteversion.3 However, recent studies have noted that up to 58% of patients with acetabular components positioned within this zone can still be at risk for dislocation.4
Some have hypothesized that abnormal spinopelvic motion could explain the relatively high dislocation rates reported with apparently well-positioned acetabular components.4-6 For example, multiple recent studies have highlighted an increased dislocation rate among patients with both a hip replacement and prior spine fusion, whose spinopelvic motion is likely impacted as a result of spine fusion.5-7 Some series report a dislocation rate in such instances that is as high as 8 to 20 percent.5-7
In this article we seek to present the current understanding of normal spinopelvic mechanics, abnormal spinopelvic mechanics, how spinopelvic motion may impact THA component positioning, and how we identify and plan for a patient with abnormal spinopelvic motion. We will present these topics in the context of a case example with abnormal spinopelvic motion.
The patient highlighted in this article is a 48-year-old male who was involved in a motor-vehicle collision over 10 years ago in which he sustained an L3 compression fracture that was treated nonoperatively. Though he was not diagnosed with any hip injuries at the time of his accident, he gradually developed right groin pain in the years following. He presented to arthroplasty clinic after years of activity modification, anti-inflammatories, physical therapy, and guided hip injections had proven ineffectual at maintaining relief from groin pain. Initial AP pelvis and hip radiographs demonstrated severe osteoarthritis of the right hip (Kellgren-Lawrence grade 4) (Figure 1). After a discussion of risks, benefits, and alternative options, he elected to proceed with THA. Standing and sitting lateral pelvic radiographs were obtained to investigate his spinopelvic mobility and overall lumbar alignment prior to surgery.

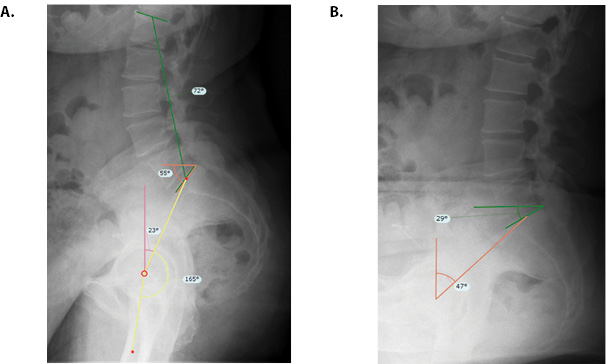
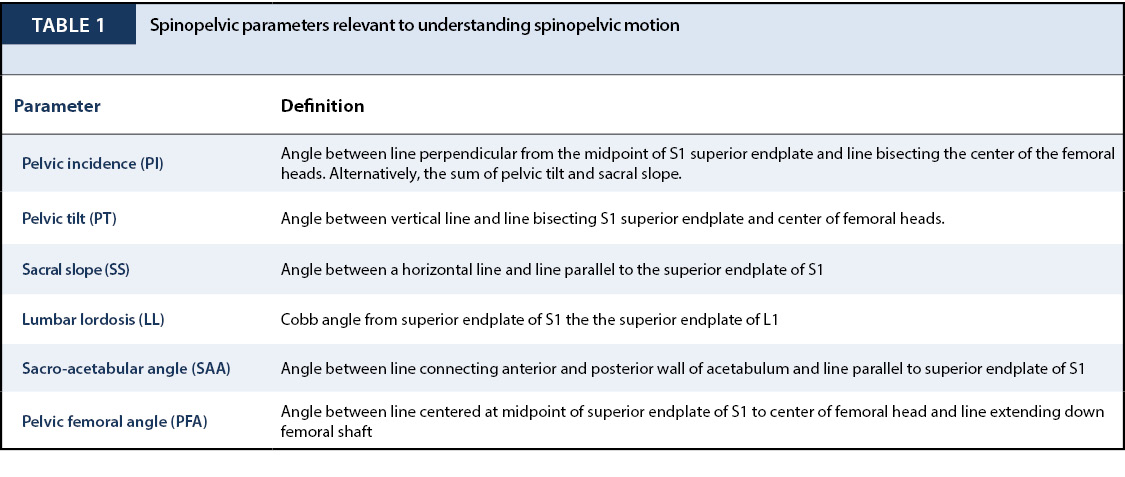
The spine parameters that have shown importance in understanding acetabular component positioning and instability include pelvic incidence (PI), sacral slope (SS), pelvic tilt (PT), lumbar lordosis (LL), sacro-acetabular angle (SAA), and pelvic femoral angle (PFA) (Table 1, Figure 2A). It is vital to have a fundamental understanding of these parameters when discussing spinopelvic mobility.
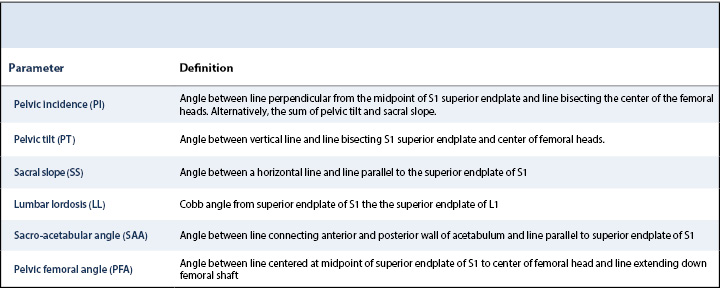
PI, the angle formed between a line drawn perpendicular from the midpoint of the S1 superior endplate and a line bisecting the center of the femoral heads, is an anatomic parameter that is constant beyond 18 years of age (Table 1). PI is related to both PT and SS through the equation (PI = PT + SS).9-11 PI is also directly related to lumbar lordosis (e.g. a high PI is associated with high lumbar lordosis).12 While PI and LL are related, as we age this relationship is less strict. The change in this relationship can be predicted through the equation [LL = 32.9 + 0.6 x PI –(0.23 x age)], which quantifies the increased kyphosis of the lumbar spine with age.13,14
PT is defined as the angle between a vertical line and a line bisecting the S1 superior endplate and the center of the femoral heads (Table 1, Figure 2A). SS represents the angle between a horizontal line and a line parallel to the superior endplate of S1 (Table 1, Figure 2A). Both PT and SS change with position and thus these markers can be used to assess for stiffness (Figure 2). Stiffness has been defined as a change in SS from sitting to standing of less than or equal to 10 degrees.10 LL represents a Cobb angle from the superior endplate of S1 to the superior endplate of L1 (Table 1, Figure 2A). Men and women have different normal values for this measurement with women having greater overall lordosis in the lumbar spine.15
Sacro-acetabular angle represents the angle between a line connecting the anterior and posterior wall of the acetabulum and the line parallel to the superior endplate of S1 (Table 1). Similar to PI, SAA does not change with position.16-19 Unlike PI, SAA takes acetabular anteversion into account and thus is used more frequently among arthroplasty discussions.20 Acetabular inclination, the angle between the horizon line and a line bisecting the anterior and posterior acetabulum can be measured on standing and sitting lateral radiographs. This value is related to SAA but can be used to quantify spinopelvic stiffness similar to the way that SS and PT are.
Pelvic femoral angle is a marker of the femur position on a lateral view (Table 1). The angle is created by a line centered at the midpoint of the superior endplate of S1 to the center of the femoral head and a second line extending from the center of the femoral head distally down the femoral shaft.
In a standing position the sacrum is tilted anteriorly. This anterior tilt is associated with LL of approximately 33 ± 12 degrees.21
Compared to standing, when supine, the pelvis further tilts anteriorly and lumbar lordosis is increased even more. While this change results in some acetabulum retroversion the overall change in pelvic tilt is less than 5 degrees between a recumbent and standing position and thus has an overall small impact on hip stability.22
Conversely, the change in PT observed moving from a standing position to a seated position is associated with a wide arc of motion.16-19 In the process of sitting, lumbar lordosis decreases and the pelvis tilts posteriorly; in turn, the acetabulum rotates posteriorly into a position of increased anteversion and increased inclination. During this process approximately 20 degrees of posterior PT can be observed.16-19 For every degree of posterior PT, the acetabular anteversion is increased by approximately 0.7-0.8 degrees.23 Additionally, this posterior pelvic tilt allows for decreased femoral flexion than would otherwise be necessary to sit (Figure 2).8-11
Disordered spinopelvic movement can be broadly placed into two categories: stiffness and hypermobility. This disordered movement leads to compensatory and, sometimes, deleterious movement at the hip. As the majority of pelvic motion occurs in the transition from sitting to standing and vice versa,16-19 we will focus on this transition. While a pelvis with normal motion undergoes 20 degrees of posterior tilt in the transition from standing to sitting, a pelvis with disordered motion does not.16-19 Such a pelvis can have either too little motion (i.e. stiffness) or too much motion (i.e. hypermobility)
Stiffness
Spinopelvic stiffness (i.e. rigidity) as it relates to the hip was popularly identified and defined by Phan et al.11 Stefl et al. provided further detail and specifically defined spinopelvic stiffness as less than 10 degrees of motion of the pelvis (as measured by change in SS) from sitting to standing and vice versa.10 There are many etiologies of stiffness such as prior lumbar fusion, ankylosing spondylitis, diffuse idiopathic skeletal hyperostosis, degenerative disc disease, and lumbar spondylosis. In general, spinopelvic stiffness necessitates increased movement of the femur at the hip to facilitate the sit-to-stand transition and vice versa. However, a stiff spine can have vastly different implications on the specific movements and limitations of the hip depending on the pelvic orientation around which stiffness occurs.
A pelvis that never achieves a SS of less than 30 degrees is considered to be overly anteriorly tilted or ‘stuck standing’.10,22 A pelvis that is ‘stuck standing’ does not achieve the posterior tilt that regularly occurs when transitioning to a sitting position. Two processes occur as a result of this lack of posterior tilt. First, the femur must hyperflex to facilitate sitting. Second, the acetabulum does not undergo normal physiologic transitional anteversion (0.8 degrees per 1 degree of posterior tilt23) that accompanies the stand to sit transition. The risks of femoral hyperflexion and decreased acetabular anteversion are impingement anteriorly and posterior hip dislocation.10,11,22 Indeed, other authors such as Heckmann et al. have implicated the ‘stuck standing’ pathology in late-presentations of posterior total hip dislocations.24
Conversely, a pelvis that never achieves a sacral slope greater than 30 degrees is considered to be overly posteriorly tilted or ‘stuck sitting’.10 Such a pelvis does not achieve the anterior tilt that physiologically occurs in the transition from sitting to standing. Its acetabulum does not undergo the physiologic retroversion that it normally would when transitioning from sit to stand.10,11 The femur itself must hyperextend to compensate for the relative lack of anterior pelvic tilt. Thus, such a hip is prone to posterior impingement and anterior hip dislocations.10,11
It is also possible for abnormal spinopelvic motion to exist in a pelvis with normal anatomic sacral slope.10,11 Such a pelvis does achieve a sacral slope of 30 degrees at some point in a transition from sitting to standing.10 In this case, impingement and dislocation are theoretically not as large of risks. However, it should be remembered that a stiff spine and pelvis still necessitate overall increased femoral movement to facilitate the sitting to standing transition. Thus, even when the spine and pelvis are well balanced, spinopelvic stiffness alone induces greater range of motion to the femur (and theoretically increases the risk of wear and dislocation).
Hypermobility
Spinopelvic hypermobility is defined by Stefl et al. as SS that changes more than 30 degrees in the sit to stand transition and vice versa.10 Contrary to stiffness, spinopelvic hypermobility means that the femur undergoes a lesser range of motion when transitioning from sit to stand than it would without spinopelvic hypermobility. Thus, some have argued that spinopelvic hypermobility may be protective with regard to THA dislocation rates.22 However, it is important to remember that anteversion and inclination of the acetabulum are directly related to spinopelvic motion. As a result, spinopelvic hypermobility also induces increased acetabular anteversion and inclination in the seated position, which can theoretically increase wear.22 Normal variant spinopelvic hypermobility may be found in young patients and in female patients.22 Conversely, pathologic hypermobility (which may be accompanied by lumbar kyphosis) often occurs among patients with extremely stiff hips,22 with a body mass index (BMI) of >40 kg/m2,25 or with neuromuscular imbalance such as in a patient with Parkinson’s disease.16-19
Overall spinal balance is fundamentally key when evaluating a patient for THA. Although there are a myriad of different spinal imbalances, most of the spinopelvic mobility literature focuses on the distinction between a lumbar spine that is in kyphosis (and more specifically, a lumbar spine with fixed sagittal plane imbalance) versus a lumbar spine that is not. Kyphosis is defined in different ways by different authors. Stefl et al. consider the lumbar spine to be pathologically kyphosed if the sacral tilt is < 5 degrees when sitting.10 Phan et al. consider lumbar kyphosis to be pathologic most pertinently in fixed sagittal plane imbalance, which they define as PI-LL > 10 degrees.11 In their article regarding workup of abnormal spinopelvic mobility patients, Luthringer and Vigdorchik seem to agree with Phan et al. and separate patients into those who do not have fixed sagittal plane imbalance and those who do (PI-LL > 10 degrees).26
The categorization of abnormal spinopelvic motion and lumbar sagittal alignment as it relates to THA has been attempted by numerous authors. Most authors focus on how hip–spine considerations affect cup positioning goals. Two manuscripts that focus on these considerations are presented below.
Phan et al.
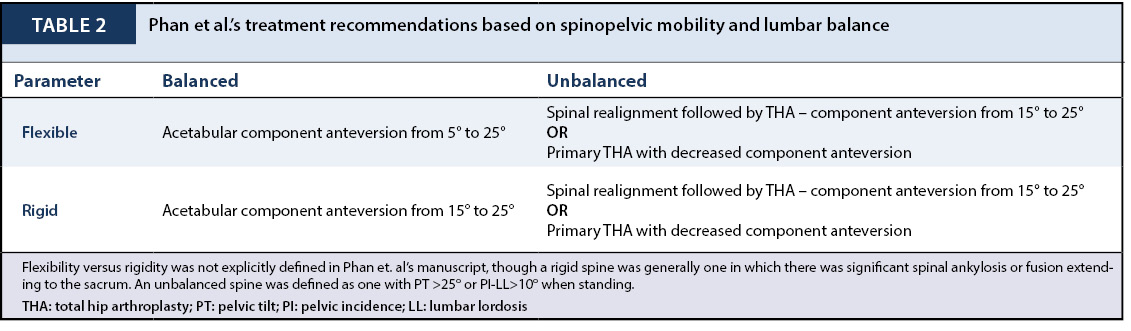
Phan et al. utilized two variables to create four categories of spinopelvic motion and lumbar balance in their systematic review of the literature (Table 2).11 The first variable was a ‘balanced’ versus ‘unbalanced’ spine. Balance was defined as a pelvic tilt < 25 degrees when standing in addition to PI-LL < 10 degrees.11 A lack of balance was defined as a pelvic tilt > 25 degrees or a PI-LL > 10 degrees.11 The second variable was flexibility versus rigidity of the spine from sitting to standing (i.e. spinopelvic mobility). Spinal rigidity was not specifically defined in this article. Rather, the authors stated that their recommendations regarding spinal rigidity were based on patients with "significant spinal ankylosis or spinal fusion extending to the sacrum."11 With these two variables at play, Phan et al. created four categories of hip-spine patients (Table 2)11:
- Flexible and balanced
- Rigid and balanced
- Flexible and unbalanced
- Rigid and unbalanced
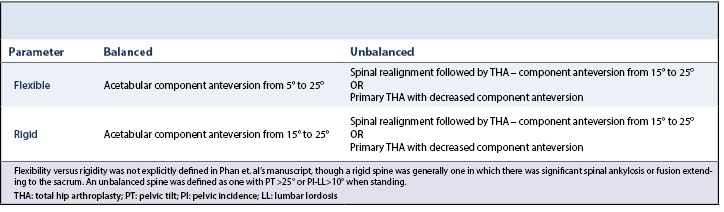
Flexible and balanced patients were considered to have normal physiologic anatomy and, therefore, the proposed goal for acetabular component anteversion was the standard 5–25 degrees proposed as Lewinnick’s ‘safe zone’.3 Rigid and balanced patients were thought to lack the ability of the pelvis to posteriorly tilt during sitting, thus creating a relative lack of anteversion and need for femoral hyperflexion to facilitate sitting. The acceptable range of cup positioning in such patients was proposed to be narrower and more skewed towards anteversion to prevent anterior impingement, levering, and posterior hip dislocation. Specifically, the cup positioning was proposed to be 15-25 degrees.11 Regardless of spine flexibility or rigidity, Phan et al. provided the same recommendations for any patient with an ‘unbalanced’ spine. The authors listed two possible options for such patients. The first was for initial spinal realignment to create a rigid and balanced spine; after this procedure subsequent THA would occur with a cup positioning goal that reflected the newly created rigid and balanced spine (i.e. 15-25 degrees of anteversion).11 Phan et al. did not specify the time between spinal realignment and THA.11 The second possibility was for primary THA with decreased component anteversion, though the authors did not specify the amount that this anteversion should be decreased.11
Luthringer and Vigdorchik
Luthringer and Vigdorchik utilized the concepts popularized by Phan et al. to provide more detail and share their entire preoperative work-up of a patient with hip–spine pathology prior to THA.26 Inherent to their recommendations is their definition of the anterior pelvic plane (APP) as it relates to the functional pelvic plane (FPP). The APP is defined by a line from the anterior superior iliac spine (ASIS) to the anterior inferior iliac spine (AIIS) on a perfect standing lateral radiograph. The FPP is defined by the coronal plane of the body while standing. The APP approximates the FPP when there is relatively normal lumbar balance. With patients who have significant lumbar kyphosis, however, the APP and FPP are significantly different because the pelvis is tilted out of the coronal plane.26 This distinction is important because the functional cup anteversion, which is a better approximation of physiologic anteversion, is better defined by the FPP; whereas surgeons generally calculate cup anteversion based on the APP when the patient is supine or lateral on the operating room table.
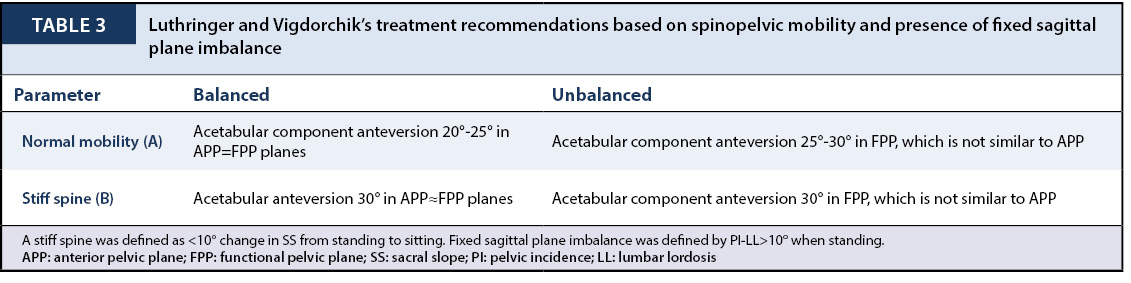
Similar to Phan et al., Luthringer and Vigdorchik focus on two variables when categorizing the hip-spine patient: the presence of fixed sagittal plane imbalance (i.e. lumbar kyphosis) and the presence of spinopelvic rigidity.26 They define fixed sagittal plane imbalance as PI-LL > 10 degrees on standing lateral radiographs; they define a stiff spine as a < 10 degree change in SS from sit to stand.26 These two variables again create four categories of hip-spine patients (Table 3):
- 1A. Normal spinal alignment with normal spinal mobility
- 1B. Normal spinal alignment with a stiff spine
- 2A. Fixed sagittal plane imbalance with normal spinal mobility
- 2B. Fixed sagittal plane imbalance with normal spinal mobility
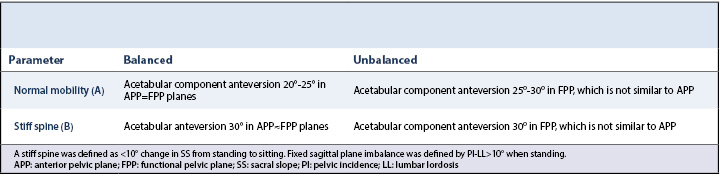
Their treatment algorithm differs depending on group affiliation. Group 1A patients (normal alignment and normal mobility) have a cup anteversion target that approximates native acetabular anatomy: 20-25 degrees of anteversion in the APP/FPP planes, which are similar.26 Group 1B patients (normal alignment with a stiff spine) have a cup anteversion target of 30 degrees in the APP/FPP planes, which are similar.26 This increased anteversion target is akin to the increased anteversion proposed by Phan et al. in rigid and balanced patients.11 It is proposed to prevent anterior impingement and posterior hip dislocations.11sup class="supComma">,26 Group 2A patients (fixed sagittal plane imbalance with normal mobility) have a cup anteversion target of 25-30 degrees in the FPP, which is significantly different than the APP in such a patient.26 It is vital to understand that the functional anteversion in such patients is projectionally lesser in the APP. Group 2B patients (fixed sagittal plane imbalance with a stiff spine) have a cup anteversion target of 30 degrees in the FPP, which is again significantly different than the APP in such patients.26
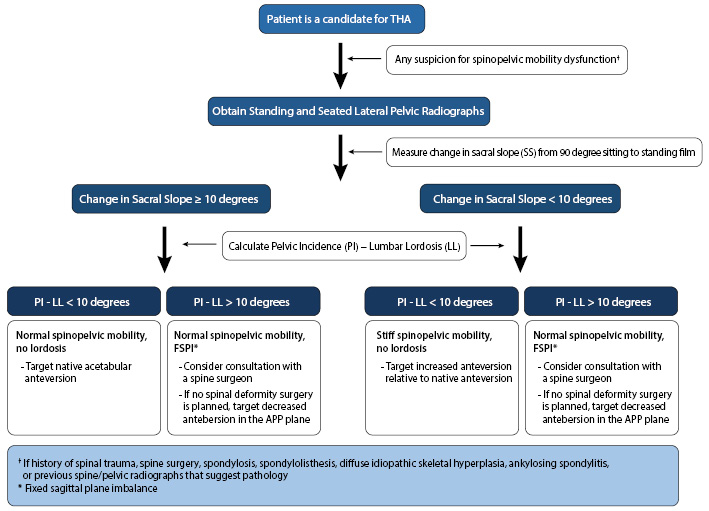
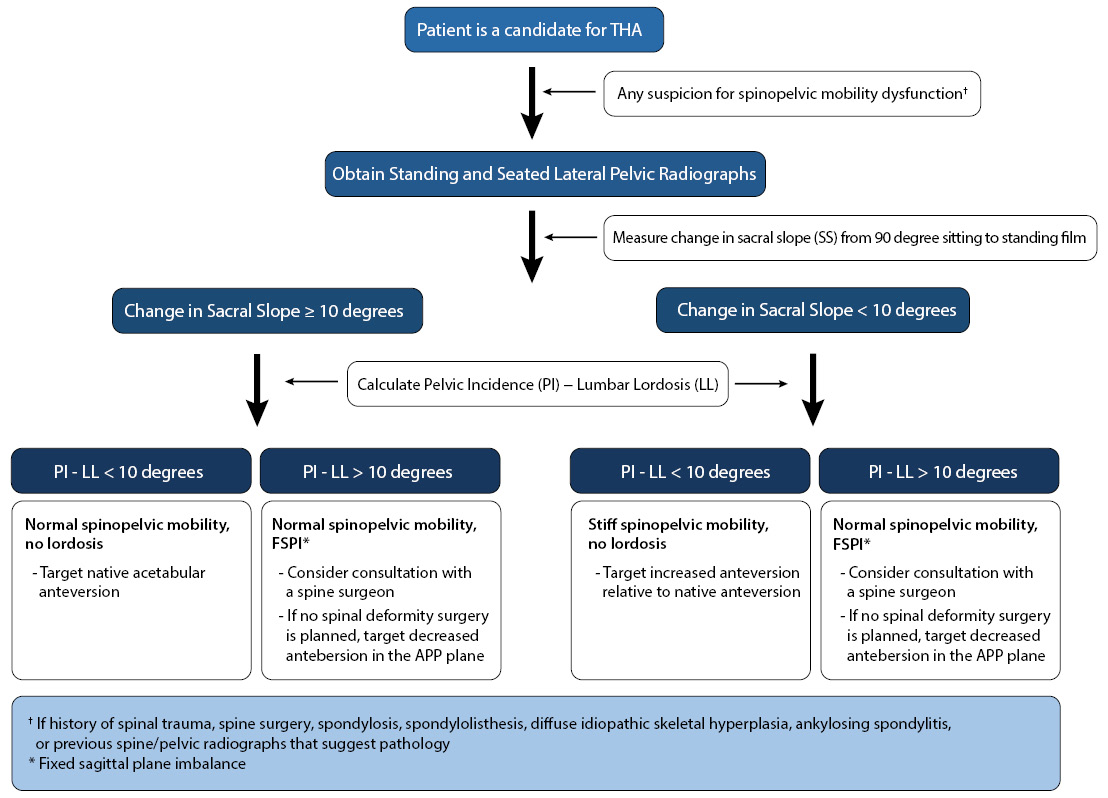
A high index of suspicion must be paid for any patient with possible spine pathology prior to THA. Based on all of the above definitions, categorizations, and proposed strategies for the hip–spine patient, we have compiled an algorithm to consider prior to THA (Figure 3). First, a focused history must be performed to elicit any evidence of spinal trauma, spinal deformity, spinal surgery, spondylosis, spondylolisthesis, ankylosing spondylitis, or diffuse idiopathic skeletal hyperplasia. If no history of any of the above is elicited, care must still be paid to the AP pelvis and lateral hip radiographs that are routinely performed in the initial evaluation for THA for evidence of any spinopelvic pathology. There should be a very low index of suspicion to rule out hip–spine pathology and/or spinopelvic mobility dysfunction. Among patients in whom hip–spine pathology may be at play, we obtain sitting and standing lateral radiographs that include the femur, pelvis, and lumbar spine. Based on Luthringer and Vigdorchik's categorizations and treatment strategies for hip–spine patients, we determine SS upon sitting and standing as well as PI and LL.26 These patient-specific parameters can be used to calculate PI-LL and change in SS, which may be used to categorize patients according to Luthringer and Vigdorchik's hip-spine definitions (Table 3). An arthroplasty surgeon may want to consider consultation with a spine surgeon prior to THA for any patients with fixed sagittal plane imbalance, although Luthringer and Vigdorchik and Phan et al. differ on this recommendation. Notably, specific cup anteversion targets as are suggested by both Phan et al. as well as Luthringer and Vigdorchik are not well characterized in the literature. As such, our cup anteversion targets are fairly generalized (Figure 3).
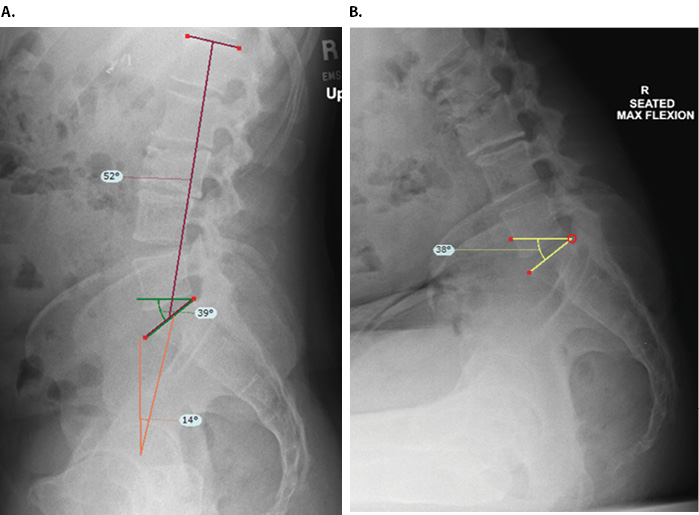
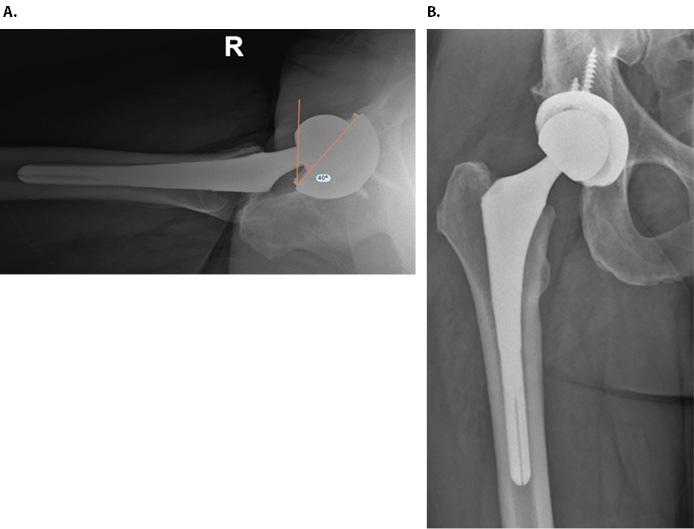
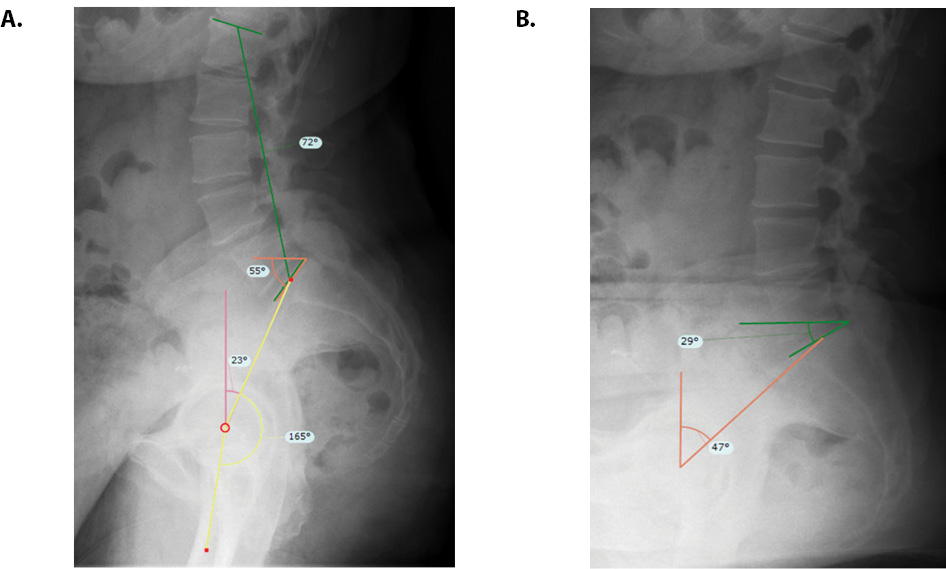
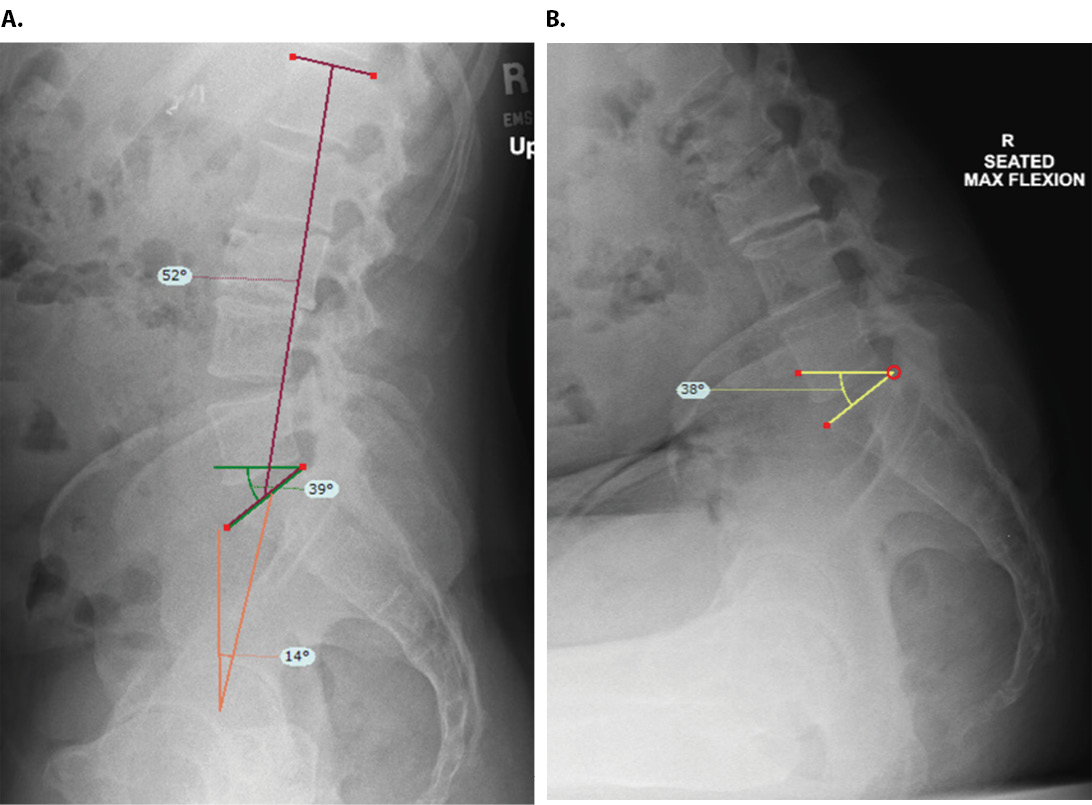
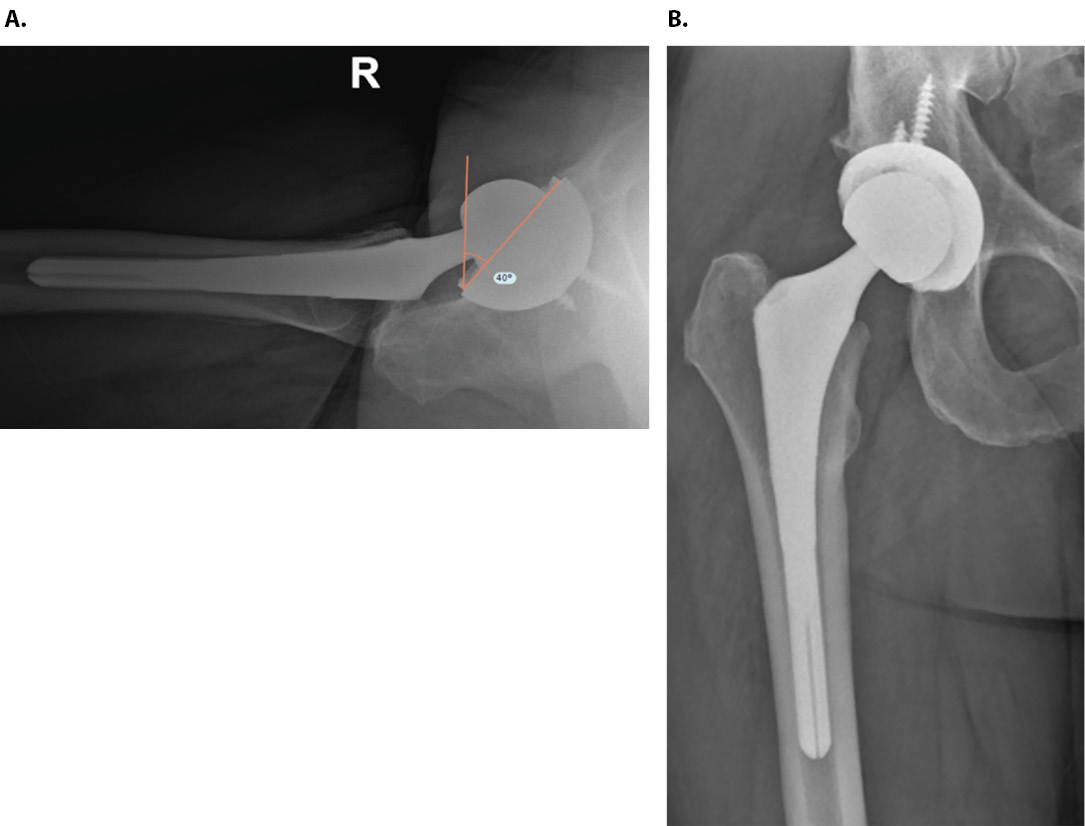
Standing and 90-degree hip flexion seated lateral radiographs were obtained to elucidate the patient’s spinopelvic mobility and lumbar balance (Figure 4). SS while standing was found to be 39 degrees (Figure 4A). PT while standing was found to be 14° (Figure 4A). PI, as calculated by adding SS and PT, was 53 degrees. LL was 52 degrees (Figure 4A). SS while sitting was found to be relatively unchanged from standing SS at 38 degrees (Figure 4B). Change in SS (absolute value of SS while sitting minus SS while standing) was found to be 1 degrees. PI-LL was 1 degrees. Phan et al. would categorize this patient as ‘rigid and balanced.’ Luthringer and Vigdorchik would categorize him as ‘normal alignment with a stiff spine.’ As the patient’s SS is never less than 30 degrees, Stefl et al. would state he is ‘stuck standing.’ Regardless of categorization, his pelvis does not achieve the normal physiologic posterior tilt that is needed to accommodate sitting. When sitting, his femur must hyperflex at his hip while his acetabulum does not achieve a normal physiologic increase in anteversion. This combination puts him at risk of anterior impingement and posterior hip dislocation. As such, our surgical goal was to give this patient significantly more cup anteversion than he would otherwise receive. He underwent THA via posterior approach. Anteversion was determined based on intraoperative markers. His postoperative films demonstrate a right THA with 40 degrees of cup anteversion (Figure 5). He is now roughly 1.5 years status post his THA. He has sustained no complications and is satisfied with the results of his hip replacement surgery.
The spine, pelvis, and hip are integrally connected. Spinopelvic mobility and overall spinal alignment are becoming increasingly recognized as causes of complications following THA. This manuscript serves to recapitulate the current understanding of this topic based on the current body of literature and to provide one case example of how this topic has affected our clinical practice. Further study is necessary in order to elucidate the proper work-up and management strategies for patients with abnormal spinopelvic motion.











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}