
Impact of Patient Age on Patient Reported Outcome Measures Following Arthroscopic Rotator Cuff Repair
Sravya Vajapeyajula, MD, Kirsten D. Garvey, MS, Elizabeth G. Matzkin, MD
The authors report no conflict of interest related to this work.
©2019 by The Orthopaedic Journal at Harvard Medical School
 PDF
PDFBACKGROUND Rotator cuff disease is a common cause of shoulder pain and disability. While not all rotator cuff tears require surgical intervention, arthroscopic repair of rotator cuff tears have been shown to result in good outcomes (i.e. decreased pain and increased function) and reduction in cost to society. Determining factors associated with poor outcomes such as age can help guide more accurate patient expectations regarding surgery. The purpose of this study was to examine the relationship between patient age at the time of the surgery and patient reported outcome measures after rotator cuff repair.
METHODS This was a prospective study consisting of three patient cohorts who have undergone rotator cuff repair from 2013 through 2016: those less than 55 years of age, those of 55-69 years of age, and those of 70 years of age or older. Data were collected at several time points following surgery including 2 weeks, 6 weeks, 3 months, 6 months, 1 year, and 2 years. Statistical analysis was performed to compare patient reported outcome measures among the three age groups preoperatively and postoperatively.
RESULTS Patients in all three age groups experienced statistically significant improvements from baseline to 1 and 2-years postoperative in pain, ASES, SANE, SST, and VR-12 after undergoing rotator cuff repair (p=<.0001).
CONCLUSION There was no effect of patient age on patient reported outcome measures following arthroscopic rotator cuff repair. Patients greater than 70 years of age did just as well as younger patients after rotator cuff repair on standardized outcome-measurement tools assessing shoulder pain, function, and overall health.
LEVEL OF EVIDENCE Level II Prospective Cohort Study
KEYWORDSRotator cuff repair, patient reported outcomes, age, elderly
Rotator cuff disease affects millions of patients every year and commonly causes shoulder pain and disability.1 Rotator cuff tears are often related to advancing age; Kim et al. found that when 237 asymptomatic shoulders were screened with ultrasonography, approximately 20% of the participants aged 60-69 years had a rotator cuff tear compared to 40.7% of subjects older than 70 years.2 Other factors associated with higher likelihood of having a rotator cuff tear are history of trauma, smoking, family history, and heavy labor.3 While the presence of a rotator cuff tear does not always lead to disability, those who are symptomatic can experience significant pain, sleep deprivation, loss of strength, limitation in performing activities of daily living (ADLs), restriction of leisure activities, inability to carry out work-related duties, and negative emotional side effects.4
Rotator cuff tears pose a considerable burden on society, and physical therapy is usually the preferred initial treatment recommendation. For those who have failed physical therapy, arthroscopic rotator cuff repair is a well-established technique with satisfactory clinical outcomes. Although Mather et al. showed that rotator cuff repair is cost-saving for society in younger patients and cost-effective for all patient groups,5 literature suggests that some patients continue to have pain despite surgery.6 Therefore, evaluating factors that predispose patients to higher rates of residual postoperative pain is important in setting more accurate preoperative expectations regarding surgical outcomes.
There is conflicting evidence in the literature regarding age and its correlation with outcomes after rotator cuff repair. While some studies suggest that older patients have lower postoperative functional and pain scores,7-10 others have shown that there is no difference in outcomes in younger versus older patients undergoing rotator cuff repair.11 The primary aim of this study was to determine whether a patient’s age affects patient reported outcome measures after rotator cuff repair. We hypothesized that older patients undergoing rotator cuff repair would perform no differently on standardized outcome-measuring tools used to assess patients’ recovery compared to younger patients undergoing rotator cuff repair.
Approval by the institutional review board was obtained prior to the initiation of the study. This was a prospective cohort study consisting of 1,144 patients who underwent arthroscopic rotator cuff repair, after failing all nonoperative treatment measures, from 2013-2016 by a total of three surgeons. After review of current literature on age associations with rotator cuff repair outcomes, we divided patients into three cohorts based on age at the time of surgery:
- Group I (< 55 years)
- Group II (55-69 years)
- Group III (70+ years)
All participants were administered a preoperative survey consisting of the following outcome-measuring tools:
- Visual Analog Scale (VAS)12 to measure overall pain level
- Veterans Rand 12-Item Health Survey (VR-12)13, a standard self-reported global health measure tool to assess a patient’s overall perspective of their health
- American Shoulder and Elbow Surgeons Shoulder Score (ASES)14 to measure functional limitations and pain of the shoulder
- Pre-operative form consisting of four questions regarding their expectations of recovery
- Single Assessment Numeric Evaluation (SANE)15 shoulder score to determine a patient self-assessment of their shoulder function
- Simple Shoulder Test (SST)16 to assess functional disability of the shoulder based on 12-item score card
The same outcome measures were reassessed at 3 months, 6 months, 1 year, and 2 years postoperatively. Interim surveys were sent at 2 weeks and 6 weeks assessing VAS pain and pain medication use.
The scores for all functional assessment metrics were tallied for each cohort at each of the time points of data collection pre- and post-operatively. The analytic sample for each analysis included subjects who had 1- or 2-year data available. Descriptive statistics are presented for baseline characteristics. The Chi-Square test or Kruskal-Wallis test were used to test for age group differences in baseline characteristics for categorical and continuous variables, respectively. Linear mixed effects models were used to assess the association between age group and outcome over time. Models were adjusted for baseline covariates that were imbalanced between the age groups.
Patient Characteristics
There were statistically-significant differences among the three age groups in terms of smoking status, workman’s compensation status and mean body mass index (BMI) (Table 1). Smoking status and workman’s compensation status imbalances were adjusted for in the analysis.
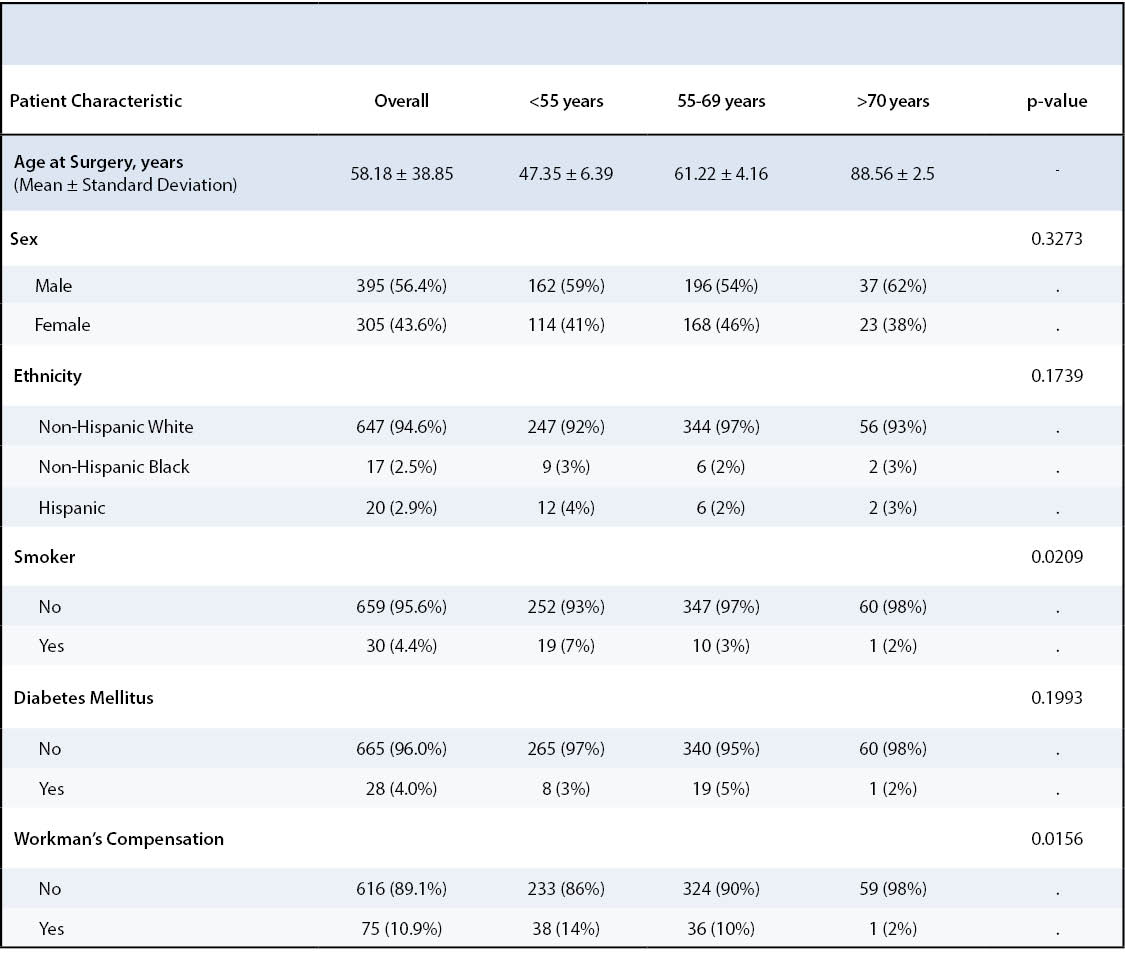
There were a total of 473 patients in Group I, 578 patients in Group II, and 93 patients in Group III who underwent rotator cuff repair during the data collection period. All patients were administered the preoperative and postoperative surveys at each of the study time points. Response rate ranged from 46% to 58% for Group I, 50% to 63% for Group 2, and 48% to 67% for Group III for each of the surveys at the end of Year 2. The analytic cohort consisted of patients who completed either 1- or 2-year follow-up. For the analytic cohort, Group I had a total of 276 patients, Group II had 364 patients, and Group III had 61 patients. Clinical characteristics of each group were assessed to evaluate rotator cuff tear size, acuity, duration of symptoms, tendon quality, and tear thickness. Much of the tear size data was missing in the database, making comparisons difficult, as such, we have included this as a limitation.
Postoperative Pain
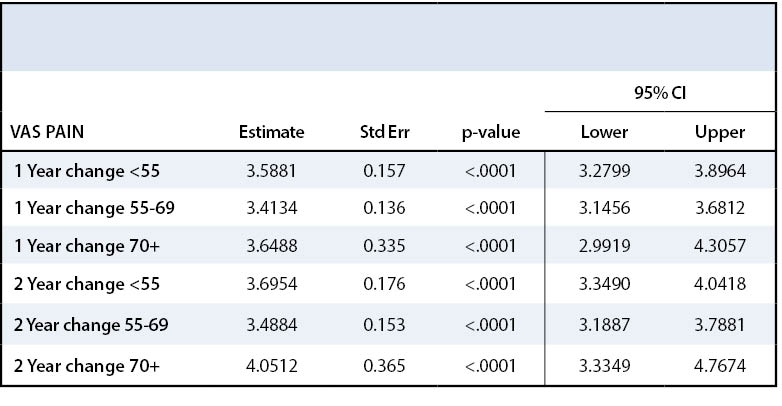
Patients in all three groups experienced a statistically significant improvement in pain after undergoing rotator cuff repair (p=<.0001) (Table 2). Patients in Group I had an average pain rating of 4.9 on the VAS before surgery and 1.3 two years postoperatively. Patients in Group II had an average pain rating of 4.6 before surgery and 1.2 at the end of second postoperative year. Patients in Group III had an average pain rating of 5.2 before surgery and 0.9 two years after surgery. All three age groups’ VAS scores postoperatively meet the Minimal Clinically Important Differences (MCID) for this measure. Tashjian et al. reported a minimum change of 3 points on a 10-point VAS scale to be clinically significant in patients treated for rotator cuff disease.17 Patients across all three age groups saw similar magnitude of pain improvement after rotator cuff repair. These results are summarized in Appendix 1, Figure 1.
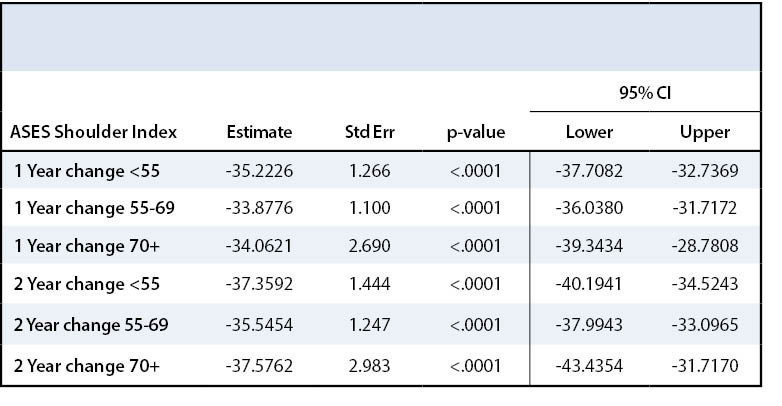
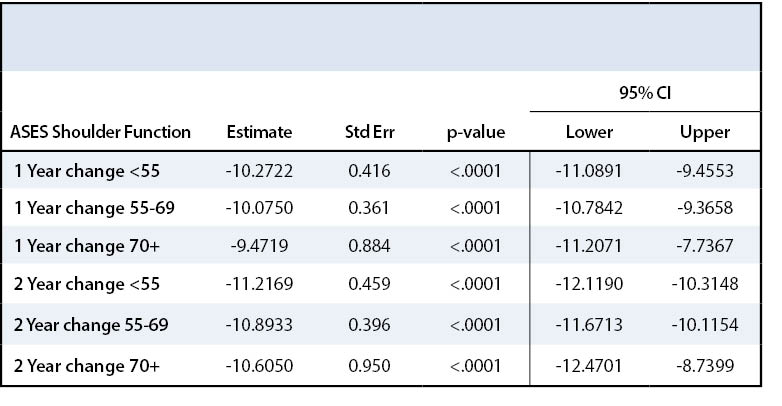
This overall improvement in pain was noted across all three groups with surgery on the ASES assessment tool as well. All three age groups experienced a statistically significant improvement in ASES shoulder index scores over time (p<.0001) (Table 3). Patients in Group I improved by 38 points, Group II by 35.4 points, and Group III by 41 points two years after surgery compared to preoperative baseline for ASES shoulder index score. All age groups met the MCID value for the ASES pain index score as described by Tashjian et al.18 All three age groups experienced a statistically significant improvement in ASES shoulder function scores over time (p<.0001) (Table 4). Patients in Group I improved their ASES function score by 11.5 points, those in Group II by 10.9 points, and those in Group III by 11.7 points by the end of two year follow up. None of the groups met the MCID value for ASES function score which would be a 12.03-point increase.18 These results are displayed in Appendix 1, Figure 2.
Postoperative Function
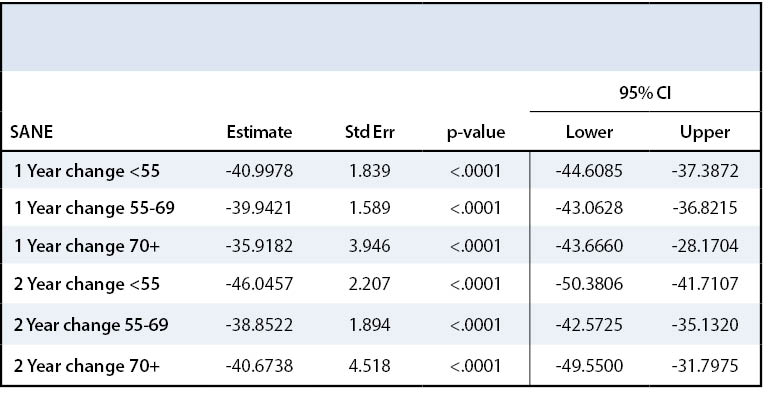
All patients demonstrated improvement in shoulder function after rotator cuff repair. SANE and SST were used to assess functional disability experienced by patients due to rotator cuff tear. All three groups experienced a statistically significant increase in SANE score after surgery (p<.0001) (Table 5)—Group I SANE score increased by 47 points, Group II by 38.6 points, and Group III by 43.7 points two years after surgery compared to their preoperative baseline (Appendix 1, Figure 3). All three groups met the minimal important difference value for SANE score, namely at least a 27.25-point increase.19
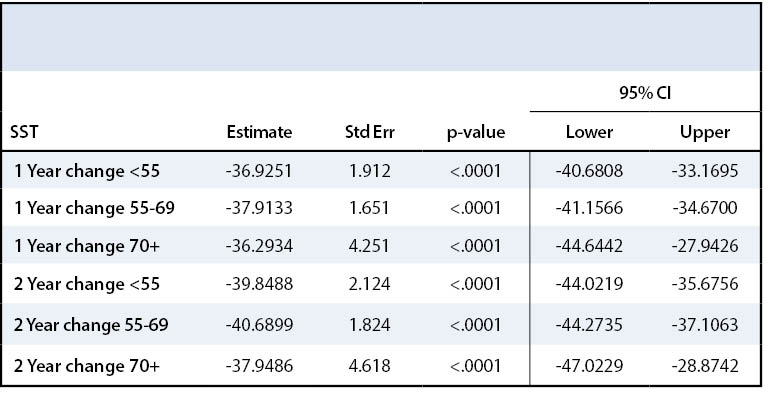
Similarly, SST score also approximately doubled after surgery across all three age groups. Group I SST increased by 40.6 points, Group II by 45.1 points, and Group III by 64.9 points two years postoperatively. All three groups experienced a statistically significant increase in SST score after surgery (p<.0001) (Table 6). All Groups met the MCID value for SST score.18 While Groups I and II saw the most improvement one year after surgery, Group III continued to see improvement in shoulder function even after Year 1 (Appendix 1, Figure 4).
Overall Health Assessment
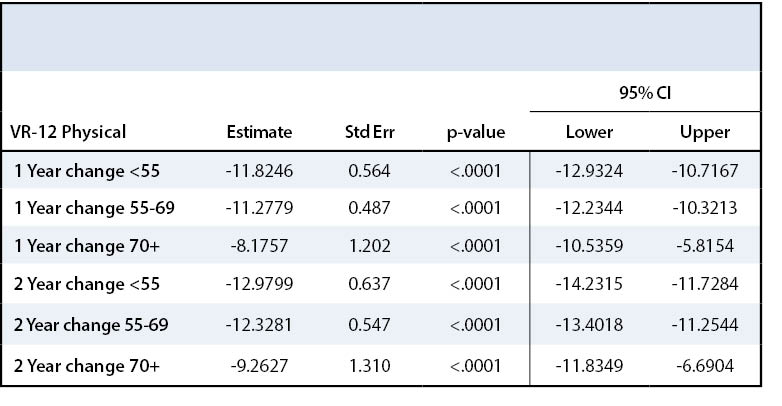
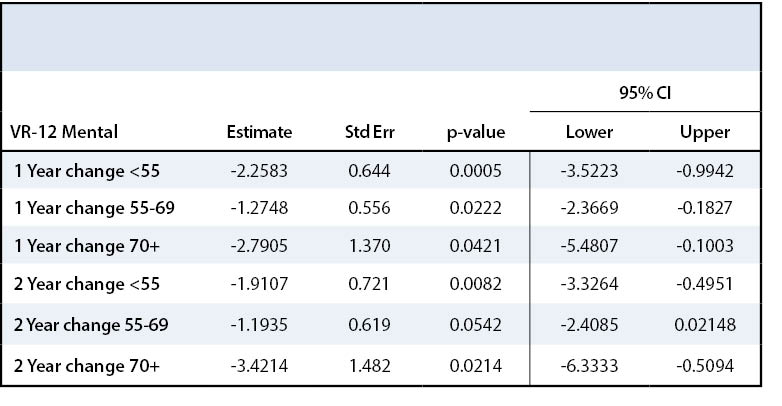
VR-12 form was used to assess patients’ overall health. The VR-12 form consisted of a series of questions about mental health, emotional health, physical health, and social functioning. The VR-12 is separated into a physical component score (PCS) and a mental component score (MCS). The higher the score, the better the patient’s perception of their overall health. All three groups demonstrated statistically significant improvement in the VR-12 PCS after rotator cuff repair (p<.0001) (Table 7). From pre-treatment to two years postoperative, Group I VR-12 PCS increased by 17.2 points, Group II by 13.6 points, and Group III by 12.8, all reaching the minimal important difference value of a 2.57-point change.19 All three groups also significantly improved in the VR-12 MCS from pre-treatment to two years postoperative (Table 8). Group I saw a 2.1-point increase, Group II a 1.4-point increase and Group III a 3.5-point increase. Groups I and III met the minimal important difference for VR-12 MCS with a point increase of at least 1.87 points.19
The incidence of rotator cuff tears increases with age. With more elderly patients opting for surgical treatment in the recent years, there has been some debate about outcomes after rotator cuff repair in this patient population. Prior studies have shown that those aged 65 years or older are predisposed to larger tears, which can be associated with higher risk of tendon degeneration and increased difficulty of repair.20 Furthermore, older patients are also more likely to have multiple medical comorbidities like diabetes mellitus, which can interfere with wound healing and immune response.21 Due to these factors and others, it has been theorized that perhaps older patients may not do as well as younger patients in terms of function and pain after rotator cuff repair. However, evidence in the literature has been contradictory.
A recent retrospective study by Chung et al. showed that health-related quality of life (HRQL) score after rotator cuff repair was negatively correlated with age in multivariate analysis.7 Despite this negative correlation, the overall HRQL score improved on average across all ages after rotator cuff repair.7 Another retrospective study by Tashjian et al. found that increased age was associated with lower healing rate as assessed by ultrasound after double-row rotator cuff repair.9 Despite this negative correlation, there was significant improvement in VAS score, ASES score, and other outcome-measurement tools compared to baseline after rotator cuff repair.9 Furthermore, Park et al showed in their systematic review that structural integrity after rotator cuff repair did not affect final clinical outcome and patients older than 75 years of age saw significantly improved clinical outcomes after rotator cuff repair.22
Our study results corroborated the results of these prior studies. We found that patients across all age groups experienced statistically significant improvement in pain and function after rotator cuff repair. There was significant improvement in VAS, ASES, SST, VR-12 and SANE scores after surgery compared to patients’ preoperative baseline. Furthermore, we also found that patients can continue to see improvement in these scores up to two years after surgery. Interestingly, we noted that patients older than 70 years of age had a greater point increase in VR-12 score one year after surgery compared to their younger cohorts. The VR-12 score represents patients’ self-reported assessment of their overall mental, emotional, and physical health. It is unclear whether this statistically significant difference in VR-12 score improvement translates to clinically significant difference. Nevertheless, our results show that rotator cuff repair in elderly patients results in very favorable outcomes.
One of the weaknesses of our study is that our study results, like with any survey results, are subject to nonresponse bias. The response rate was 74%. A potential limitation to this study is that we did not assess which of the non-responders had expired during the study period. Therefore, the population of non-responders could include those subjects that had passed. Additionally, we aimed to evaluate any significant differences in clinical characteristics including tear size, acuity, duration of symptoms, tendon quality and tear thickness, but many of the data were missing from the database, limiting further analysis of these variables beyond descriptive statistics. A final limitation was our inability to adjust for BMI due to incomplete data.
There was no effect of patient age on clinical outcomes after rotator cuff repair. Older patients did just as well as younger patients after rotator cuff repair on standardized outcome-measurement tools assessing shoulder pain, function, and overall health.






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}